Would Science have killed the New Normal, how long before the masks fall off?
Publié le
Most non-pharmacological coercive measures taken to combat Covid-19 lack a solid scientific basis or evidence of proven effectiveness. In the long term, however, they would constitute a factor of psychological abuse for many citizens and are contrary to the constitution. We come back here to the case of masks, which we will develop and specify, and show, with scientific studies, that a reduction of the measures more respectful of the psychological health and the fundamental rights of the persons could be taken. This relief would not seem to impact the safety of everyone. We finally propose a summary sheet at the end of the article which is also available in PDF format here.
Here are, first of all, some essential points, which science has proven in one year, and which change the game, but which still seem to be too widely ignored or misunderstood:
Asymptomatic people have too low a viral load to be contagious(1) (on the other hand, carriers who will have symptoms, and who will therefore be identifiable, are contagious over a short period of time called presymptomatic. Presymptomatic carriers do not cough, coughing being the mechanism of contamination from which the mask mainly protects) (2)(3)(4)(5)(6)(7)(8)(9). The contagious asymptomatic hypothesis is tantamount to saying that every healthy person is an unknowing sick person or is presumed to be guilty. Remember that this assumption is the basis of the generalized mask. It is undoubtedly, also, an argument to justify the confinement of the whole population. The invalidation of this contagious asymptomatic hypothesis may explain, in part, the lack of positive correlation observed in real life of containment on the decrease of hospitalizations and deaths by more and more scientific studies, and now in America where states that are completely open and unrestricted, such as Texas for many weeks, are seeing a dramatic drop in cases and deaths over the same period.
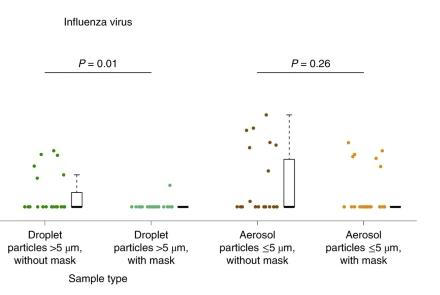
The virus is spread by fine aerosol droplets which pass through the pores of the mask which are up to 1000 times larger than the virus (Fig. 1, the more efficient FFP2 masks filter a part of the aerosols larger than 600 nm, the virus is 60 to 140 nm) and would propagate even beyond the social distances (10). This aerosol-type transmission, which could also explain the phenomenon of supercontaminants, increasingly seems to be the main mode of transmission(11)(12)(13)(14) . Fortunately, there is the notion of threshold(15): 1 virus is not enough, it takes many more to be contaminated(16)(17)(18)(19) .
Fig. 1 Respiratory droplets collected for 30min while not wearing (dark green) or wearing (light green) a surgical face mask, and aerosols collected for 30min while not wearing (brown) or wearing (orange) a face mask, collected from individuals with acute respiratory symptoms who were positive for influenza virus. Data from [11] Respiratory virusshedding in exhaled breath and efficacy of face masks, Nature Medicine volume 26, pages 676–680 (2020).
What are the implications?
All scientific studies and observations confirm it(20)(21)(22)(23) , the risk of Covid-19 contamination outdoors is extremely low. It takes about 1 million viruses per ml in our bronchial tubes to reach the threshold for SARS-Cov‑2 (24)(25)(26)(27) . This threshold cannot be reached by aerosols outside, it is a question of volume(28).
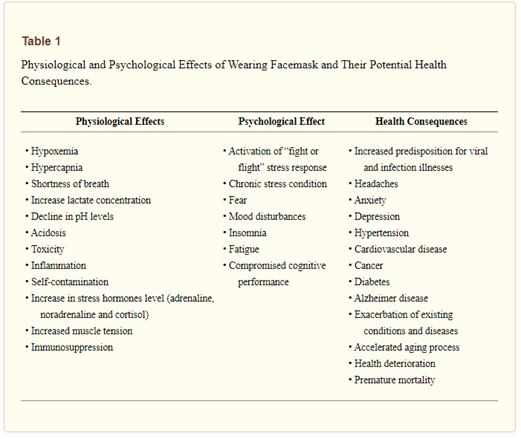
Another case is that of children who are rarely symptomatic and therefore not very contagious(29)(30). Wearing a mask outdoors or for children seems to be done in spite of any benefit-risk balance and common sense. Because if the scientific evidence for the usefulness of the mask generalized to the whole population is lacking (31)(32)(33)(34)(35)The risks of its negative impact on physical and mental health have been demonstrated, for example (36)(37)(38)(39)(40) and Table 1. Masking, confinement, social distancing, and the associated stress and isolation can further weaken our immune system (41)(42)(43)and could therefore contribute to increase, paradoxically, the risk of severe forms (and therefore much more contagious), hospitalizations, deaths and contagions, especially in populations that are not at risk for which the benefit of these measures is not demonstrated (44)(45)(46)(47)(48)(49)(50)(51). It could also be useful to think about reinforcing your immune system with vitamin D, C and Zinc and why not a little essential oil of Noble Laurel or Ravintsara (52), for example in case of a more risky contact.
Indoors, aerosol contamination is possible if there is insufficient ventilation. Typically, you would need to be in contact with a high viral load person for a sufficiently long time (typically > 10 minutes. Mask and social distancing would have little effect, except for symptomatic coughers (53)(54)(55)(56)(57)(58) who should be isolated and masked, preferably with a FFP2 mask, in case of essential displacement. A standard mask offers no real protection against aerosols smaller than 3 um (59)(60)(61) and even a FFP2 mask, which is less breathable, offers only imperfect protection, and real-life protection depends greatly on the conditions of use (62)A better solution would be ventilation or air purification (there are for example very efficient HEPA, ozone, and UVC filters) so that the threshold is never reached indoors.
https://youtu.be/mrXBinu3Swo : Wearing a mask outdoors is useless! « Dr. Blachier, studies to back it up! April 26, 2021.
In conclusion, if according to the WHO (63)(64), the wearing of a medical mask type FFP2 (non-medical masks would have a limited efficiency and could even increase the risks of infection if badly used(65)) is useful for health care personnel in direct contact with patients, symptomatic patients and also undoubtedly for people at risk as an additional protection, the generalized wearing of it for people with no apparent symptoms of the disease has little or no scientific justification (66)(67)(68)(69)(70)(71). The WHO, after having pronounced itself against (72)seems to accept it (73)because of the strong demand of the states to reassure the populations, as a measure rather of a psychological nature (74)or even a talisman that reassures(75)and despite the low contagiousness of asymptomatic (76)(77)(78)(79)(80)(81)(82)(83). A recent article from MIT calls into question social distancing, since transmission by aerosol would therefore cross these distances(84). If science seems to have killed the new normal, how long will it be before the masks come off?
Aryan Afzalian
Civil engineer and Doctor of Applied Sciences. Researcher specialized in the field of atomistic quantum physics applied to the modeling of nano- and bio-electronics and author of the site https://auxamescitoyennes.com/
Nour de San
Independent consultant. Doctor of Medicine, specialized in clinical biology (immunology and microbiology), formerly responsible for risk management in discovery and development of the Vaccine unit of GSK. Project Manager in support of the COVID crisis management at Erasmus Hospital from April 2020 to May 2021.
Florence Parent
MD — PhD, Public Health and Medical Education, author of books on Medical Education.
Martin Zizi
MD-PhD, Biophysicist, Professor of Physiology (KULeuven and VUB), former Epidemiological Director of the Department of Defense, former Scientific Director and Chairman of the Ethics Committee, former UN Advisor on Biological Disarmament and Unscom Bio-Inspector.
Mask Summary Sheet:
Covid-19: Wearing the mask what do the scientific studies say:
This note is for information purposes only. It is based on the scientific literature and an interpretation of the benefit-risk balance. It aims to help everyone to better understand the mechanisms of transmission and to know the benefits and risks of wearing a mask, in the hope that each person can use this knowledge to best protect themselves. It does not take into account, nor is it intended to substitute for the legal jurisdiction specific to each country, but is intended as a message to the authorities asking them to consider that measures more respectful of the psychological health and fundamental rights of people could be taken. This relief would probably not impact everyone’s safety.
I wear the mask, I am :
Un Malade avec Symptôme: Nécessaire 👍 (Je protège les autres de mes exhalations directes: gouttelettes de salive quand je tousse par exemple).
Le Personnel soignant directement au chevet des malades: Nécessaire 👍 (Je me protège des exhalations directes des malades).
Une Personne ne présentant aucun symptôme : 👎 Inutile (Pas d’efficacité prouvée, asymptomatiques pas contagieux 1 , risques prouvés sur la santé physique et mentale et affaiblissement du système immunitaire, risque si mauvaise utilisation).
Une personne à risque et qui a peur: 👍 utile avec modération ( Porter le masque, de préférence FFP2, comme précaution ultime et pour se rassurer peut faire sens surtout dans les lieux clos quand les distanciations sociales ne sont pas possibles. Dès que possible, je l’enlève pour ne pas risquer d’affaiblir inutilement mon système immunitaire. Je pense d’ailleurs à renforcer ce dernier par de la vitamine D, C et du Zinc et pourquoi pas un peu d’huile essentielle de Laurier Noble ou de Ravintsara, par exemple si j’ai eu un contact plus à risque (Je demande bien conseil à un professionnel de santé, par ex. mon pharmacien ou mon médecin de famille pour les dosages et utilisations).
What does the mask protect from, what doesn’t it protect from?
It protects me if a symptomatic sick person with a high viral load coughs directly on me, which represents a very small proportion of contaminations.
The mask does not protect me from indirect contamination via the hands, nor does it protect me from contamination by fine aerosol droplets that pass through the pores of the mask (up to 1000 × larger than the virus; indoors, the FFP2 type mask filters out some of the aerosols). These are the main modes of contamination. Fortunately, there is the notion of a threshold (85).
Notes et références
La fenêtre de contagion du Covid est d’environ 2 jours avant à 5 jours après l’apparition des premiers symptômes de la maladie, on parle respectivement de malades présymptomatiques et symptomatiques. Il n’y a que durant cette période qu’une personne présente une charge virale suffisante pour être contagieuse. Les asymptomatiques ont eux une charge virale trop faible (environ 20 × moindre), et plusieurs études ont montré l’absence de transmission des asymptomatiques, même à leur proches au sein du foyer familial, et cela avec ou sans masque. C’est bien entendu lié à la notion de seuil développé ci-dessous. Les présymptomatiques, eux, typiquement ne toussent pas, ils peuvent contaminer notamment par aérosols pour lesquels le masque est inefficace.
World Health Organization. Advice on the use of masks in the community, during home care and in health care settings in the context of the novel coronavirus (2019-nCoV) outbreak. Geneva, Switzerland; 2020. https://apps.who.int/iris/handle/10665/330987
World Health Organization. Advice on the use of masks in the context of COVID-19. Interim guidance 5 June 2020. https://apps.who.int/iris/handle/10665/332293 : Many countries have recommended the use of fabric masks/face coverings for the general public. At the present time, the widespread use of masks by healthy people in the community setting is not yet supported by high quality or direct scientific evidence and there are potential benefits and harms to consider (see below).
A study on infectivity of asymptomatic SARS-CoV‑2 carriers, Respir Med. 2020 Aug; 169: 106026. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7219423/: 455 contacts who were exposed to the asymptomatic COVID-19 virus carrier became the subjects of our research. The median contact time for patients was four days and that for family members was five days. All CT images showed no sign of COVID-19 infection. No severe acute respiratory syndrome coronavirus 2 (SARS-CoV‑2) infections was detected in 455 contacts by
nucleic acid test. In summary, all the 455 contacts were excluded from SARS-CoV‑2 infection and we conclude that the infectivity of some asymptomatic SARS-CoV‑2 carriers might be weak.
Contact Settings and Risk for Transmission in 3410 Close Contacts of Patients With COVID-19 in Guangzhou, China. https://www.acpjournals.org/doi/10.7326/M20-2671: Infection max dans foyer (10x plus que à l’hôpital et 100x plus que dans transport en commun) et augmente fortement avec la force des symptomes (asymptomatiques 10 à 20 fois moins contagieux) et la toux.: Among 3410 close contacts, 127 (3.7% [95% CI, 3.1% to 4.4%]) were secondarily infected. Of these 127 persons, 8 (6.3% [CI, 2.1% to 10.5%]) were asymptomatic. Of the 119 symptomatic cases, 20 (16.8%) were defined as mild, 87 (73.1%) as moderate, and 12 (10.1%) as severe or critical. Compared with the household setting (10.3%), the secondary attack rate was lower for exposures in health care settings (1.0%; odds ratio [OR], 0.09 [CI, 0.04 to 0.20]) and on public transportation (0.1%; OR, 0.01 [CI, 0.00 to 0.08]). The secondary attack rate increased with the severity of index cases, from 0.3% (CI, 0.0% to 1.0%) for asymptomatic to 3.3% (CI, 1.8% to 4.8%) for mild, 5.6% (CI, 4.4% to 6.8%) for moderate, and 6.2% (CI, 3.2% to 9.1%) for severe or critical cases. Index cases with expectoration were associated with higher risk for secondary infection (13.6% vs. 3.0% for index cases without expectoration; OR, 4.81 [CI, 3.35 to 6.93]).
Analysis of Asymptomatic and Presymptomatic Transmission in SARS-CoV‑2 Outbreak, Germany, 2020, EID Journal, 27 (4), April 2021, https://wwwnc.cdc.gov/eid/article/27/4/20–4576_article: We determined secondary attack rates (SAR) among close contacts of 59
asymptomatic and symptomatic coronavirus disease case-patients by presymptomatic and symptomatic exposure. We observed no transmission from asymptomatic case-patients and highest SAR through presymptomatic exposure. Rapid quarantine of close contacts with or without symptoms is needed to prevent presymptomatic transmission.
Coronavirus Disease Outbreak in Call Center, South Korea, EID Journal,Volume 26, Number 8—August 2020: https://wwwnc.cdc.gov/eid/article/26/8/20–1274_article#r6: We describe the epidemiology of a coronavirus disease (COVID-19) outbreak ina call center in South Korea. We obtained information on demographic characteristics by using standardized epidemiologic investigation forms. We performed descriptive analyses and reported the results as frequencies and proportions for categoric variables. Of 1,143 persons who were tested for COVID-19, a total of 97 (8.5%, 95% CI 7.0%–10.3%) had confirmed cases. Of these, 94 were working in an 11th-floor call center with 216 employees, translating to an attack rate of 43.5% (95% CI 36.9%–50.4%). The household secondary attack rate among symptomatic case-patients was 16.2% (95% CI 11.6%– 22.0%). Of the 97 persons with confirmed COVID-19, only 4 (1.9%) remained asymptomatic within 14 days of quarantine, and none of their household contacts acquired secondary infections. Extensive contact tracing, testing all contacts, and early quarantine blocked further transmission and might be effective for containing rapid outbreaks in crowded work settings.
Cheng H, Jian S, Liu D, et al. Contact Tracing Assessment of COVID-19 Transmission Dynamics in Taiwan and Risk at Different Exposure Periods Before and After Symptom Onset. JAMA Intern Med. 2020;180(9):1156–1163. doi:10.1001/jamainternmed.2020.2020:
https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2765641 : In this case-ascertained study of 100 cases of confirmed COVID-19 and 2761 close contacts, the overall secondary clinical attack rate was 0.7%. The attack rate was higher among contacts whose exposure to the index case started within 5 days of symptom onset than those who were exposed later. Among the 91 close contacts of the 9 asymptoma tic cases, no secondary transmission was observed.
Post-lockdown SARS-CoV‑2 nucleic acid screening in nearly ten million residents of Wuhan, China Étude sur les asymptomatiques PCR-positifs à Wuhan. Cao et al, dans la revue Nature https://www.nature.com/articles/s41467- 020–19802‑w
A guideline to limit indoor airborne transmission of COVID-19, M. Z. Bazant and J. W. M. Bush: PNAS April 27, 2021 118 (17) e2018995118; https://doi.org/10.1073/pnas.2018995118 MIT study on airborne transmission.
idem
https://www.cidrap.umn.edu/news-perspective/2020/04/commentary-masks-all-covid-19-not-based-sound-data. : Pas vraiment d’évidence pour le masque pour tous, surtout que risque de transmission par aérosol.
Respiratory virus shedding in exhaled breath and efficacy of face masks https://www.nature.com/articles/s41591-020‑0843‑2: Intérêt du masque pour gouttelette chez symptomatiques, chez asymptomatiques faibles différences surtout pour transmission aérosol qui est observée pour les coronavirus.
COVID-19 transmission—up in the air The Lancet Respiratory Medicine Crossref DOI link: https://doi.org/10.1016/S2213-2600(20)30514–2 Published: 2020-12 : Respiratory viruses are transmitted in three main ways. First, contact transmission, where someone comes into direct contact with an infected person or touches a surface that has been contaminated. Second, through droplet transmission of both large and small respiratory droplets that contain the virus, which would occur when near an infected person. Third, through airborne transmission of smaller droplets and particles that are suspended in the air over longer distances and time than droplet transmission. Initially it was thought that airborne transmission of SARS-CoV‑2 was unlikely, but growing evidence has highlighted that infective microdroplets are small enough to remain suspended in the air and expose individuals at distances beyond 2 m from an infected person. This knowledge is also corroborated by investiga tion of spread of cases between people who were not in direct or indirect contact, suggesting that airborne transmission was the most likely route. In July, over 200 scientists published a statement calling for international bodies to recognise the potential for airborne spread of COVID-19 as they were concerned that people would not be fully protected by adhering to the current recommendations.
La notion de seuil : 1 virus ne suffit pas, il en faut beaucoup plus pour être contaminé. Il faut 1 million de virus par ml pour le seuil de contamination au SARS-Cov‑2. Ce seuil ne peut pas être atteint à l’extérieur par aérosol, même dans une foule, c’est une question de volume d’air. A l’intérieur, il faudrait être en contact avec une personne à haute charge virale pendant suffisamment longtemps (typiquement >10 minutes). Le masque et la distanciation sociale n’y changeraient pas grand-chose (sauf pour les symptomatiques qui toussent), le plus important serait l’aération et la purification de l’air pour que le seuil ne soit jamais atteint à l’intérieur.
Wölfel R. et al. Virological assessment of hospitalized patients with COVID-2019. Nature. 2020 May;581(7809):465–469. doi : 10.1038/s41586-020‑2196‑x. Epub 2020 Apr 1. Erratum in : Nature. 2020 Dec;588(7839):E35. PMID : 32235945
Qiu X, et al. Defining the role of asymptomatic and pre-symptomatic SARS-CoV‑2 transmission, a living systematic review. 2021 Jan 20. Clin Microbiol Infect. 2021; S1198-743X(21)00038–0. doi:10.1016/j.cmi.2021.01.011
La Scola B et al. Viral RNA load as determined by cell culture as a management tool for discharge of SARS-CoV‑2 patients from infectious disease wards. Eur J Clin Microbiol Infect Dis. 2020 Jun;39(6):1059–1061. doi : 10.1007/s10096-020- 03913–9.
RAG interpretation and reporting of SARS COV‑2 PCR results (Sciensano) 20201208_Advice RAG Interpretation and reporting of COVID PCR results.pdf (sciensano.be)
Outdoor Transmission of SARS-CoV‑2 and Other Respiratory Viruses: A Systematic Review J Infect Dis. 2021 Feb 24;223(4):550–561. doi: 10.1093/infdis/jiaa742:Five identified studies found a low proportion of reported global SARS-CoV‑2 infections occurred outdoors (<10%) and the odds of indoor transmission was very high compared to outdoors (18.7 times; 95% confidence interval, 6.0–57.9). Existing evidence supports the wide-held belief that risk of SARS-CoV‑2 transmission is lower outdoors but there are significant gaps in our understanding of specific pathways.
https://www.lci.fr/sante/video-covid-19-le-port-du-masque-a-l-exterieur-est-il-utile-2162627.html: Risque de contagion très faible en extérieurs.
https://www.youtube.com/watch?v=mrXBinu3Swo : Le port du masque en extérieur ne sert à rien! » Dr Blachier, études à l’appui! 26 Avril 2021. Il dit encore: Très peu de contaminations se font en extérieur, d’après plusieurs études.On devrait dire aux gens de se retrouver dehors plutôt qu’à l’intérieur. Le port du masque en extérieur ne sert à rien! Dr Blachier – Épidémiologiste. Émission : Les Grandes Gueules Chaîne : RMC STORY / RMC (Radio).
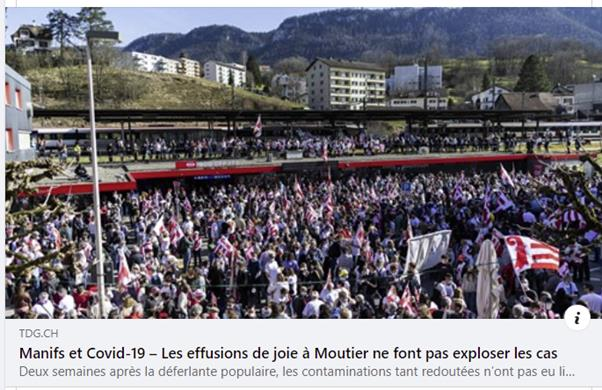
https://www.tdg.ch/les-effusions-de-joie-a-moutier-ne-font-pas-exploser-les-cas-830669237575?fbclid=IwAR11X7WwnJB7b2jF1aMOSvzbt2NkccPd9livLPi5RJDVH4BnHjjx7BzzRFM « Jacques Gerber, ministre jurassien de la Santé, le confirme: «Ce dimanche, nous avons enregistré six cas, contre une vingtaine en fin de semaine. Nous sommes clairement en descente. Il n’y a donc pas d’explosion. C’est un cas d’école.» Aucune flambée non plus à Moutier et dans le Jura bernois, avec même une diminution des cas. » (Vincent V.)
Wölfel R. et al., op. cit.
Qiu X, et al., op. cit.
La Scola B et al., op. cit.
RAG interpretation and reporting of SARS COV‑2 PCR results, op. cit.
Association between living with children and outcomes from covid-19: OpenSAFELY cohort study of 12 million adults in England, BMJ 2021; 372. (Published 18 March 2021), https://doi.org/10.1136/bmj.n628 : Among 9 334 392adults aged 65 years and under, during wave 1, living with children was not associated with materially increased risks of recorded SARS-CoV‑2 infection, covid-19 related hospital or intensive care admission, or death from covid-19. In wave 2, among adults aged 65 years and under living with children was associated with a very small increased risk, e.g., inthe number of hospital admissions of 1–5 per 10 000 people from 160 to between 161 and 165 (children aged 0–11) and with an increase of an increase of 2–6 per 10 000 (children aged 12–18 years).
https://www.lefigaro.fr/vox/societe/il-faut-urgemment-mettre-fin-au-port-du-masque-pour-les-enfants-20210525?fbclid=IwAR2x3N2f4kZHTRiOV97HosF1AGb2WlJcdZQeQmsFR3aA9F5VZN4cTkAZjDk : Masquer les enfants pour une maladie qui ne les concerne pas signifie notre défaite de la pensée et notre perte de dignité. Psychologues, pédiatres et pédopsychiatres, nous sommes nombreux à être très inquiets de la hausse des hospitalisations et des troubles que développent les jeunes enfant s depuis le premier confinement. Jusqu’à six fois plus d’admissions en pédopsychiatrie.
World Health Organization. Advice on the use of masks, op. cit.
World Health Organization. Advice on the use of masks in the context, op. cit.
Respiratory virus shedding in exhaled breath, op. cit.
MacIntyre C.R., Seale H., Dung T.C., Hien N.T., Nga P.T., Chughtai A.A. A cluster randomised trial of cloth masks compared with medical masks in healthcare workers. BMJ open. 2015;5. This study is the first RCT of cloth masks, and the results caution against the use of cloth masks. This is an important finding to inform occupational health and safety. Moisture retention, reuse of cloth masks and poor filtration may result in increased risk of infection.
Universal Masking in Hospitals in the Covid-19 Era, N Engl J Med 2020; 382:e63 DOI: 10.1056/NEJMp2006372. Article sur l’usage généralisés du masque en milieux hospitalier. We know that wearing a mask outside health care facilities offers little, if any, protection from infection. Public health authorities define a significant exposure to Covid-19 as face-to-face contact within 6 feet with a patient with symptomatic Covid-19 that is sustained for at least a few minutes (and some say more than 10 minutes or even 30 minutes). The chance of catching Covid ‑19 from a passing interaction in a public space is therefore minimal. In many cases, the desire for widespread masking is a reflexive reaction to anxiety over the pandemic. There may be additional benefits to broad masking policies that extend beyond their technical contribution to reducing pathogen transmission. Masks are visible reminders of an otherwise invisible yet widely prevalent pathogen and may remind people of the importance of social distancing and other infection-control measures.
Aerosol Filtration Efficiency of Common Fabrics Used in Respiratory Cloth Masks. https://pubs.acs.org/doi/10.1021/acsnano.0c03252.
Kao T.W., Huang K.C., Huang Y.L., Tsai T.J., Hsieh B.S., Wu M.S. The physiological impact of wearing an N95 mask during hemodialysis as a precaution against SARS in patients with end-stage renal disease. J Formos Med Assoc. 2004;103:624–628. https://pubmed.ncbi.nlm.nih.gov/15340662/ : Thirty nine patients (23 men; mean age, 57.2 years) were recruited for participation in the study. Seventy percent of the patients showed a reduction in partial pressure of oxygen (PaO2), and 19% developed various degrees of hypoxemia. Wearing an N95 mask significantly reduced the PaO2 level (101.7 +/- 12.6 to 92.7 +/- 15.8 mm Hg, p = 0.006), increased the respiratory rate (16.8 +/- 2.8 to 18.8 +/- 2.7/min, p < 0.001), and increased the occurrence of chest discomfort (3 to 11 patients, p = 0.014) and respiratory distress (1 to 17 patients, p < 0.001). Baseline PaO2 level was the only significant predictor of the magnitude of PaO2 reduction (p < 0.001). Conclusion: Wearing an N95 mask for 4 hours during HD significantly reduced PaO2 and increased respiratory adverse effects in ESRD patients.
Beder A., Buyukkocak U., Sabuncuoglu H., Keskil Z.A., Keskil S. Preliminary report on surgical mask induced deoxygenation during major surgery. Neurocirugia (Astur) 2008;19:121–126. https://pubmed.ncbi.nlm.nih.gov/18500410/ : This study was undertaken to evaluate whether the surgeons’ oxygen saturation of hemoglobin was affected by the surgical mask or not during major operations. Repea ted measures, longitudinal and prospective observational study was performed on 53 surgeons using a pulse oximeter pre and postoperatively. Our study revealed a decrease in the oxygen saturation of arterial pulsations (SpO2) and a slight increase in pulse rates compared to preoperative values in all surgeon groups. The decrease was more prominent in the surgeons aged over 35.
Ong J.J.Y., Bharatendu C., Goh Y., Tang J.Z.Y., Sooi K.W.X., Tan Y.L. Headaches Associated With Personal Protective Equipment – A Cross-Sectional Study Among Frontline Healthcare Workers During COVID-19. Headache. 2020;60:864–877. [PubMed] [Google Scholar] : Coronavirus disease 2019 (COVID-19) is an emerging infectious disease of pandemic proportions. Healthcare workers in Singapore working in high-risk areas were mandated to wear personal protective equipment (PPE) such as N95 face mask and protective eyewear while atten ding to patients. Most healthcare workers develop de novo PPE-associated headaches or exacerbation of their pre-existing headache disorders.
Notes et présentation de l’intervention du Dr Vanden Bossche au Sommet sur la vaccination qui a eu lieu dans l’Ohio entre le 1 et le 3 mars 2021, organisé par le Biogate Scientific Center Pvt Ltd.
Kieran Dee, Daniel M Goldfarb, Joanne Haney, Julien A R Amat, Vanessa Herder, Meredith Stewart, Agnieszka M Szemiel, Marc Baguelin, Pablo R Murcia, Human rhinovirus infection blocks SARS-CoV‑2 replication within the respiratory epithelium: implications for COVID-19 epidemiology, The Journal of Infectious Diseases, 2021;, jiab147, https://doi.org/10.1093/infdis/jiab147: Virus-virus interactions influence the epidemiology of respiratory infections. However, the impact of viruses causing upper respiratory infections on SARS-CoV‑2 replication and transmission is currently unknown. Human rhinoviruses cause the common cold and are the most prevalent respiratory viruses of humans. Interactions between rhinoviruses and co-circulating respiratory viruses have been shown to shape virus epidemiology at the individual host and population level. Here, we examined the replication kinetics of SARS-CoV‑2 in the human respiratory epithelium in the presence or absence of rhinovirus. We show that human rhinovirus triggers an interferon response that blocks SARS-CoV‑2 replication. Mathematical simulations show that this virus-virus interaction is likely to have a population-wide effect as an increasing prevalence of rhinovirus will reduce the number of new COVID-19 cases.
Masks Are Neither Effective Nor Safe: https://pdmj.org/papers/masks_are_neither_effective_nor_safe/index.html : A Summary Of The Science A review of the peer-reviewed medical literature examines impacts on human health, both immunological, as well as physiological. The purpose of this paper is to examine data regarding the effectiveness of facemasks, as well as safety data. The reason that both are examined in one paper is that for the general public as a whole, as well as for every individual, a risk-benefit analysis is necessary to guide decisions on if and when to wear a mask.
World Health Organization. Advice on the use of masks, op. cit.
World Health Organization. Advice on the use of masks in the context, op. cit.
A study on infectivity of asymptomatic SARS-CoV‑2 carriers, op. cit.
Contact Settings and Risk for Transmission in 3410 Close Contacts of Patients With COVID-19 in Guangzhou, op. cit.
A guideline to limit indoor airborne transmission of COVID-19, op. cit.
COVID-19 transmission—up in the air The Lancet Respiratory Medicine Crossref DOI, op. cit.
Respiratory virus shedding in exhaled breath and efficacy of face masks, op. cit.
MacIntyre C.R., Seale H., Dung T.C., Hien N.T., Nga P.T., Chughtai A.A., op. cit
Universal Masking in Hospitals in the Covid-19 Era, op. cit.
World Health Organization. Advice on the use of masks, op. cit.
World Health Organization. Advice on the use of masks in the context, op. cit.
idem
Universal Masking in Hospitals in the Covid-19 Era, op. cit.
World Health Organization. Advice on the use of masks, op. cit.
World Health Organization. Advice on the use of masks in the context, op. cit.
A study on infectivity of asymptomatic SARS-CoV‑2 carriers, , op. cit.
Contact Settings and Risk for Transmission in 3410 Close Contacts of Patients With COVID-19 in Guangzhou, op. cit.
Analysis of Asymptomatic and Presymptomatic Transmission in SARS-CoV‑2 Outbreak, , op. cit.
Coronavirus Disease Outbreak in Call Center, South Korea, op. cit.
Cheng H, Jian S, Liu D, et al., op. cit.
Post-lockdown SARS-CoV‑2 nucleic acid screening in nearly ten million residents of Wuhan, , op. cit.
A guideline to limit indoor airborne transmission of COVID-19, , op. cit.
La notion de seuil : 1 virus ne suffit pas, il en faut beaucoup plus pour être contaminé. Il faut 1 million de virus par ml pour le seuil de contamination au SARS-Cov‑2. Ce seuil ne peut pas être atteint à l’extérieur par aérosol, même dans une foule, c’est une question de volume d’air. A l’intérieur, il faudrait être en contact avec une personne à haute charge virale pendant suffisamment longtemps (typiquement >10 minutes). Le masque et la distanciation sociale n’y changeraient pas grand-chose (sauf pour les symptomatiques qui toussent), le plus important serait l’aération et la purification de l’air pour que le seuil ne soit jamais atteint à l’intérieur.
FREE JOURNALISM IS EXPENSIVE.
To make articles, reports, interviews, videos... Help us: subscribe, subscribe family, friends, talk about us, make a donation.