Fact-checking the fact-checkers — The Source (April 4, 2021)

Prof dr. Martin Zizi, former President of the Ethics Committee and of the Commission for Medical Ethics within the Belgian Department of Defense, in charge of the relations with the Order of Physicians between 1997 and 2004, former Scientific Director and Head of the Division of Epidemiology and Biostatistics, researcher in Molecular Biology and Biophysics; he was an advisor/expert for the Belgian authorities, the EU and the UN.
This article is a response to the publication « Do PCR tests overestimate Covid-19 cases? » — published in the new « fact checking » section of La Libre Belgique.
In a Democracy, the press must control the power in place and not the citizens. The solution: a true testing policy without exclusivity and based on reality, not on a « rubber band » that keeps us all in fear and allows us to decide anything.
Recently, an article mentioned me in a fact-checking column (The Source, a new column in La Libre) about PCRs and their misuse throughout this SARS2 crisis. I find the intention commendable and I share the desire of the Editor-in-Chief and the journalist. However, reading the article, I believe that the result is not nearly informative enough, the conclusion being to reassure about the use of PCR and to contrast it with other types of tests. As announced in a previous article, we need to work on solutions, and this light fact-check publication gives me the opportunity to not only explain the problem to the general public, but also to outline the solution to this problem. So I have to come back to this subject because it is far too important to be diluted even with brilliance. Note that I have intervened in the press twice on this subject, and I have never said or written that RCPs had no role to play as the article describes ((1), (2), as well as numerous exchanges between La Libre and myself). I also differentiate between symptomatic and asymptomatic every time.
What is the problem with the PCR tests that have been made the cornerstone of this health, social and economic debacle? In fact, there is not one, but two perfectly distinct problems and they must be clearly distinguished.
Problem #1. PCR ≠ Infections.
This means that a positive PCR does not automatically equate to infection (a given for all molecular biologists). Germs simply live among us. For example, almost all of us have staphylococcal germs on our skin at one time or another. The frequency is between 20–30% at any given time(3), and 66% of people have this germ on their skin intermittently, but repeatedly(4). If we did PCRs on thousands of people tomorrow, we would almost always have between 30% and 66% of « positive cases » in the entire random population. How many of us have a staph infection of the skin? Almost nobody! Do you understand the problem now? So a disease is not the same as a positive PCR test. On the other hand, if we have a skin disease, then in that case, PCR can help the clinician to demonstrate that it is staphylococcus, to know if it is resistant or not, and to know if it is another germ, and in Inall cases, it will help the physician to prescribe the appropriate treatment. The context of the test is therefore absolutely cardinal.
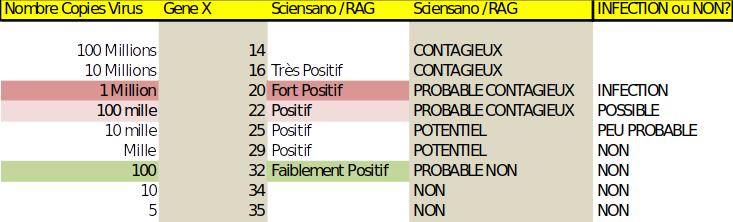
To be sick with a virus, measuring a dozen or millions of viruses per measurement — and PCR does this — means nothing if one does not understand the notion of threshold of infection . Indeed, each virus has a different threshold to make us sick; for hepatitis B this threshold is very low, but for HIV it is higher. For SARS2 we need about one million particles per milliliter in our bronchial tubes to get infected and sick(5) (references even quoted by Sciensano).
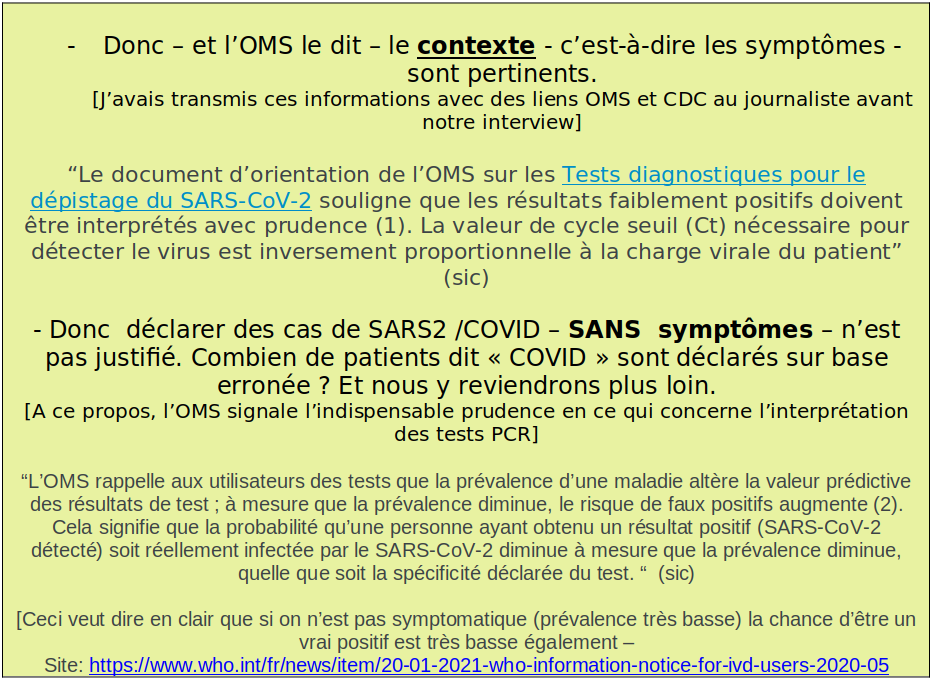
As a reminder, PCRs amplify the genetic material to be measured per cycle, each cycle doubling the mass of what is to be measured. But as with any instrument, whether in the scientific field or elsewhere (music, construction, etc.), it is necessary to start by calibrating the tool to be used. For PCR, this is equivalent to performing a detection of a series of viral solutions with a known number of particles (10 viruses/ml, 100 viruses/ml, 1000 viruses per ml, and so on). It is then possible to match these different viral concentrations to PCR multiplication cycles: 2, 3, 4 … 20, 30, 40 cycles. This makes it possible to define the number of cycles necessary (the Ct or Cycle Treshold) to reach the famous threshold of one million viruses per ml (below this threshold, there is no infection). It is important that this calibration is done for all laboratories, as there are differences between the machines. Note, however, that after a very large number of cycles, any instrument will inevitably fall outside the PCR’s range of use. WHO had initially published standardized protocols at 35 cycles — then more recently reported as an addendum that each laboratory should indeed calibrate their machines (reference given in the insert). And in Belgium? We were happily doing 35 cycles, where the million per ml is reached at around 23 cycles according to our own standards (this figure fluctuating only by a few units depending on the machine used)!
Remember also that the PCR is a test that works in reverse — the longer you run the reaction, the less you measure what you’re looking for. 23 cycles give us the threshold of one million viruses per milliliter — which is necessary to say that we have a risk of infection — which is still not an infection because each of us can be more or less sensitive to the virus (another problem real but which is beyond the scope of this article). 33 cycles lead us to measure 1000 times less viruses (because 2 exponent 10 = 1024, i.e. the difference of cycles between 33 and 23), so instead of a million viruses, the sample contains only 1000! Above this threshold (called « Ct » in the PCR results) of 23, we can conclude that : This is not an infection! If you repeat these tests with too many cycles, the results become random and non-specific and are no longer reliable at all: i.e. the SAME sample could be positive once, negative once… so the test gives no valid information.
Let’s go even further: if I explain to you that in the ICU (Intensive Care Unit) in Belgium, some of these patients who have not contracted COVID are nevertheless labelled « COVID » because the test is « positive ». And this even in the absence of any clinical picture of respiratory infection sometimes!!! This can’t happen in our good kingdom? Don’t believe me, talk to the ICU nurses and doctors. So the problem of CRP extends even in part to hospital beds…
And when we know that in France and Germany, PCR is done at 38, even more than 40 cycles, in Ireland at 45 cycles (some protocols and standards were shared so comparisons are possible), we can only notice that the problem goes beyond our borders… Are you beginning to understand why this debate about PCR cycles and calibration is critical?
Problem #2. PCR ≠ Contagiousness.
A positive PCR does not equate to an infectious person. This is the ‘tail’ of the infections. The Source article does a better job on this — and I thank the reporters for their informative clarity, as they are not scientists.
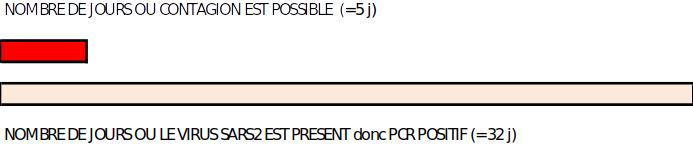
The SARS-CoV 2 virus remains in our bodies for weeks after the illness is over — so we are no longer contagious at that point. There are many publications on this subject (this point is no longer contentious at all). What the article does not highlight is that this non-contagion period is 4 to 6 times longer than the contagion period! If the « window » for concluding that someone is « dangerous to others » is a few days, then the chance of getting it wrong — that is, of testing positive while not being contaminated — is obviously much greater.
Furthermore, the fact-checking does not mention that I provided them with the Lancet which was used to introduce the subject(6)as well as another article(7) from New England Journal of Medicine that covers this topic and tries to explain how to do it better — to use the tests intelligently. Which is my goal too. The Source article mentions a scientific reference which, after studying and explaining this problem, concludes that between 50% and 75% of PCR tests are false positives for this ‘infection tail’ reason, but points out — without any data that the 75% figure is surely wrong because and I quote « We do not randomly test […] people suspected of COVID because they have symptoms or their contacts ». This quote is completely false, we will come back to it. Did the scientist questioned by the journalist of La Libre Belgique present a table with statistics? On what basis are the symptoms estimated? After clinical medical consultation or after a declaration on honour — as is permitted? Did the journalist only check the number of cycles performed in the Belgian labs?
With hindsight, it is difficult to estimate the proportion of correct versus incorrect tests, as this would have required systematic correlation of PCR, symptoms and serological tests [qui sont des tests qui mesurent les anticorps dans le sang des personnes réellement infectées] — something that was apparently not done. So we can only have an estimate based on current scientific knowledge. But if the residence period of the virus in the body is 4 to 6 times shorter than the period of contagion, we could deduce that a significant proportion of these tests do not reflect any risk of contagion. It is high time to stop the war of numbers on this subject — especially when people without symptoms are massively tested — and recognize that we don’t know… but then why present these tests as the only possibility of measurement? This raises questions.
There is a 3rd problem with these PCR tests: the huge financial stakes.
This was one of the issues that the journalists told me they were going to address in this fact-check and that they don’t even touch on in their opus. Why not? The potential conflicts of interest of some of the advisors in this area should be investigated. Search on different university sites, start-ups or companies that provide this expensive service (test statistics are published on the site of La Libre Belgique) and check possible links with experts or advisors. Controlling shareholder agreements. At a rate of 600‑2000 tests per day in peak for a small lab [données contrôlées indépendamment par téléphone], and at a price of 47 Euros, it is a lot of money. How much is it? What about a large university lab or private companies? How much is it? It would be necessary to analyze this of course, but it would not be surprising to reach figures approaching several hundred million euros just for small Belgium and for the PCRs. All this money for tests that help us so little and allow us to justify in an ad hoc way this medical, social and economic suicide?
Also, you probably don’t know this… but we’ve been there. After 9/11, my phone was constantly clogged with companies wanting to » help me manage the crisis » and so the pressure to recommend purchases of PCR machines (between 80 and 100 machines) and to push a vaccine (yikes!) against anthrax was enormous. And I have never recommended PCRs (nor this vaccine) in my capacity as an advisor to the Defense Cabinet but also to the Prime Minister’s Office and to Health (via the Intercab). Measuring anthrax by PCR was expensive and unnecessary because anthrax lives among us. As experts — and especially during crises — the commercial pressures and temptations are enormous…
There is also a side problem: false oppositions. Indeed, some people oppose PCR tests to antigenic and serological tests — for reasons of conflict of interest, and they hide them well. And I fear that the press does not understand that it is being taken for a ride. My communications do not attack PCR and do not want to promote other types of tests. I have nothing to sell, no test, no drug, and especially not — contrary to some of our experts and journalists — wind — and I am out of these activities in biotechnology which made my daily life for nearly 40 years! I only explain, and this in full agreement with the WHO, that PCR is a powerful tool for diagnostic confirmation if one is ill with symptoms. But — as the WHO points out — we have to be very careful with the conclusions if we test people who are not ill or without symptoms. I say this less politely than WHO, I agree. It’s a much-needed wake-up call — not a whisper of discomfort! I personally wrote in the press, and explained to the reporter that a testing strategy was needed and I invite readers of all my LinkedIn posts to check for themselves by giving them keywords to search. I do not give an opinion, but try to raise the debate.
About the other tests — and this makes me sad because they would save lives — it would be good if others would talk about them. Once again, the Source article does not reflect our conversation. I never told the reporter that these antigenic tests were all calibrated for this purpose. On the contrary, I explained to the journalist that these tests could be perfectly calibrated to be positive(8) only during the period when the person tested is contagious. This is a problem of the mass of chemical reagents to be put in the test kits. So I deplore the « drowning » of fish with these rates of true or false positives and comparisons made on tests that were never optimized for this period of contagion.
Finally, if we know that a test gives erroneous results for multiple reasons ((9) and (10)) and was imposed in a financial blur(11), and serves to block any debate and to break everything(12), it is not only legitimate, but even our duty to say it. It is a bit of a stretch to say that the PCR, despite its limitations, is the only screening option in light of all that has been decided and the NON-COVID deaths it has caused. Let’s call it for what it is: the bungee tests, which allow to justify everything. This debate around RCPs is TOO important to put it under the carpet, because it is on this basis that lockdowns, green or red zones, or travel control are decided… This is the same basis for calculating COVID beds in ICUs (intensive care units).
It should be noted at this point that The Source, in addition to the problems mentioned above, contradicts itself. Indeed, it reports through the mouth of Dr. L. Cornelissen that « since non-symptomatic people are not tested, there are no problems ». This is false information because asymptomatic people are tested well in Belgium and en masse. We have been testing them since the beginning, and it was publicly said by the authorities that they would stop testing during the November 2020 vacations. We officially resumed these tests at the end of November. La Libre Belgique as well as other newspapers) announced these important official decisions by important articles [see Edition of Oct. 19]. 2020, title: Turning back the clock: people without symptoms will no longer be tested]. The resumption on November 23 was announced everywhere [voir site de la RTBF en date du 14 Nov]. In this article, it does talk about asymptomatic people who have had contact and I quote [« And then, that we can track contacts and trace back the chains of asymptomatic people. »]. The chains of asymptomatic! This is not a sexually transmitted disease, but a zoonosis! So the tracing does not give a correct picture of the dispersion of this virus (and an outdoor contact will be safe compared to a contact in a closed environment) but let’s pass.
Moreover, when the PCR tests were resumed on a large scale [see La Libre Édition of Nov. 25, 2020], Commissioner Corona himself said: « […] rapid tests (he talks about PCR) are reliable in people who remain asymptomatic with a high viral load and are therefore contagious » (sic). What is the proportion of these people? In general, non-symptomatic individuals have low or no viral loads(13). In addition, travelers (the vast majority of whom have no symptoms) and even parents of children who have been in contact with a case are tested all the time, so we test one patient plus 2 other people. Furthermore, when anyone can request a test after signing a Declaration of Honor that he/she has the symptoms of COVID, it becomes surreal. As the fact-checking journalist confuses the problem of the detection threshold (problem #1) with the problem of the persistence (presence) of the virus in our respiratory tract long after there is no longer a contagious risk (problem #2). Confusing these two different problems is precisely the cause of this misuse of PCRs.
The Source also mentions another subject that I must develop: the asymptomatic
I quote The Source: « An April 2020 study in the journal Nature even estimates that 44% of infections in households occur during the pre-contamination phase, before the first symptoms appear. A trend followed by the WHO, which states that « it is mainly just before infected people develop symptoms (i.e. two days before) and at the very beginning of the disease that they are the most contagious ». I am going to surprise you, but I completely agree. Indeed, the vast majority of contaminations are made within the family bubbles and closed environments and not outside.
We are dealing with pre-symptomatic potentials and PCR has its place. However, we should stop talking nonsense and making amalgams. The majority of people with COVID who are asymptomatic are in the rest of the population, not around the patients. There have been many studies on this subject which have not been able to show a risk of contagiousness. One of the largest studies ever conducted was in Wuhan, involving nearly 11 million people(14). It shows — contrary to previous studies — that these asymptomatic people — even if they are PCR positive — emit little virus (which is logical because they are not sick and therefore do not cough!) and that their rate of contagiousness is almost zero. Why does this go unnoticed?
The problems with PCRs that I explain in this article are not new and there are examples where PCRs failed(15). The press (this does not concern La Libre belgique) reported that it was fake news so here is another much needed fact-check. In British Columbia, there was a pseudo-epidemic of SARS1 in 2003 measured by supposedly perfect PCR tests. In the end, this « epidemic » — which resulted in eight deaths, six of which were due to bacterial pneumonia — was due to another perfectly banal and benign corona. For the record, there are seven human coronaviruses (four that cause the common cold as well as SARS1, MERS, and SARS2). At the time, those in charge had the presence of mind to test the antibodies, which avoided panic and fear. In 2006 in New Hampshire (USA), an outbreak of pertussis(B. Pertussis) turned out to be a creation of PCR. This false alarm problem is known and was discussed in the Lancet in 2006(16).
If reporters were doing their job as inquiring minds, they wouldn’t have to call and drink in either incorrect or outright untruthful words from some of my ex-colleagues. All they have to do is read Sciensano’s notes — available online. It is amazing that Sciensano writes one thing and does its opposite. Lie or stupidity, the question remains as far as I am concerned, and I hope that many citizens will make the effort to ask themselves. This is controllable by anyone, does not require specialized knowledge and reveals the following facts:
And the surprises don’t stop there. Sciensano mentions in his notes on PCR(19) that:
Who are we kidding… On the one hand, Sciensano puts the right references with correct information on their website, and on the other hand, they completely ignore it and create and maintain a climate of panic fear to the decision makers and all the populations of the EU based on not correctly interpreted measurements. I don’t know about you, dear readers, but all this shocks me deeply, and isn’t it time that the Press finally does its job: Control the Power, read, understand, educate itself in order to inform.
What is the solution?
There should be a ‘testing path’ — an algorithm. I will limit myself to the basics — a real protocol/pathway will have to/will be established by experts and colleagues:
1. See patients in person, based on symptoms and clinic — and confirm the potential diagnosis of COVID by PCR. For this purpose, PCR will be very efficient.
2. For contacts — these are either pre-symptomatic if they eventually become ill, or those who will remain perfectly asymptomatic — focus mainlyon contacts in closed environments where contamination occurs (the famous bubbles, public transport, buildings with centralized ventilation… which are the best places for any virus to spread). The others do not. The mania for doing everything all the time is deleterious.
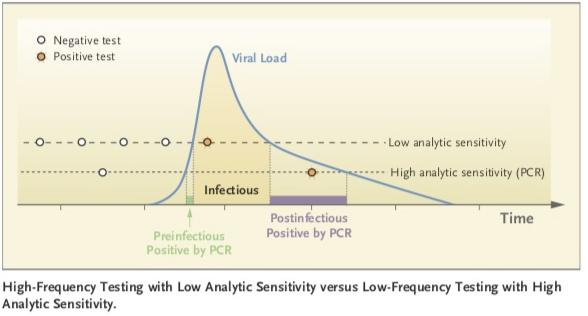
3. For the non-symptomatic — the entire population — PCR not being a suitable tool — antigenic tests perfectly calibratedto make the positive result coincide with the period of contagion. The false negative rate is defined by the chemical design of such tests — so it could be perfectly reliable. If there is any doubt, you should go see your family doctor and a PCR may follow. I also did not say that these tests were already calibrated, but that they should be and that it would not take much time. I put you a relevant reference and invite you to look carefully at the figure in the paper below. Only a test that is less sensitive than PCR could effectively match the period of contagion and identify the contagious.
4. Serological tests (which measure antibodies in the blood) should also be used. Because after more than 17 months, it is time to do a randomized serological study in correspondence with our population — as any crisis requires — because it will be the only reliable method to estimate the proportion of people infected but who remain carriers. — therefore to calculate a true IFR (Infection fatality rate). This would break the cycle of fear, and reassure the public instead of the CFR (case fatality rate) — which only measures our inability to handle COVID cases in a way that is not appropriate. This was the subject of many reports, here is one written by about 40 people under the leadership of the Hoover Institute at Stanford(20). Moreover, this report was given by me to La Libre on two occasions. So I don’t think it’s intellectually honest or a service to the public to portray myself as a detractor of PCRs, having practiced non-stop between 1993 and 2014, in part on environmental germs… Why? The question is asked.