This text extends the debate on medical and health care decision making that was initiated around Evidence-based-medicine (EBM) with the carte blanche entitled: » the role of physician training and medical epistemology in the crisis of Covid 19 (1) « . Discussion that continued in a second carte blanche, focused — as its title indicates — on a critique of the precautionary principle » Precautionary Principle or « Risk of Blame? »(2)
By(3):
» In the face of any disease, is it not our duty to care for patients? And if there is no unanimous treatment in the medical world, is that a reason to do nothing? (…) The scientists who refute this only do so on the basis of studies that are insufficient to date. Not enough to prove definitively that the treatments work, but also not enough to prove that they don’t work. And often they have no personal experience with these treatments, which they reject out of hand. Otherwise they wouldn’t be so peremptory.(4).
The « forced » desertion(5) of the front line of health care was all the more damaging because at decision-making levels closer to the field, many practitioners did not want this dissolution of their role and skills. These field caregivers are fully committed to their patients, and therefore suffer from the imposition of such a defection. Suffering is undoubtedly more essential (in the sense of the very essence) is present among front-line ambulatory health care providers with holistic approaches to care and health (general practitioners, especially those with open and integrative practices; home care nurses, etc.) and their networked extensions (psychotherapists; osteopaths; physiotherapists; alternative approaches to care such as acupuncturists, hypnotherapists, phytotherapists, etc.) and their extensions in networks (psychotherapists; osteopaths; physiotherapists; alternative approaches to care such as acupuncturists, hypnotherapists, phytotherapists, naturopaths, aromatherapists, gemmotherapists …), often organized within the framework of responsible citizen engagements. It is also a large part of the support and « care » sector that has literally « gone by the wayside », including the « caregivers » who are so precious when such projects exist, making it possible to ensure the proximity network in a health system.
We could go further in this idea of desertion and suffering of the actors of the care, which also touched the population with regard to the roles of each one in the city when all are thus « prevented from working », by referring to the work of Richard Sennett(6): « The ‘craft’ may suggest a way of life that disappeared with the advent of industrial society, but this is misleading. The craft designates an elementary and enduring human impulse, the desire to do one’s work well in itself. It goes far beyond skilled manual labor; it serves the computer programmer, the doctor and the artist; parenting improves when practiced as a skilled trade; so does citizenship. (…) Every good craftsman pursues a dialogue between concrete practices and reflection; this dialogue leads to nourishing habits, which in turn establish a rhythm between the solution and the identification of a problem.(7).
Without being able to develop, except in an introductory way with the example that will follow, the perspective of the patient-partner(8), it is clear that such a vision of care has also been swept aside. Its return, like that of emerging care practices in such an environment, if not totalitarian, in proximity to what can be called a sanitary dictatorship, was made at the price of what was lost between T0 — that is to say the moment of the beginning of the confinements — and the time of a recovery of spirits, notably in the face of the individual dramas and becoming statistics of what is euphemistically called « collateral damage » of Covid 19.
This « desertion by regulation », as we have called it, has broken in many places this vital impulse, proper to autonomy(9) and to the power of the person, notably by its operative and managerial modality, infantilizing, of which the following box gives an account in terms of care.
The confusion is particularly great when a representative of the state, and a fortiori its president, intervenes with a « hegemonic benevolence », as the humanitarian emergency can do for the populations of Africa when they are supposed to be « beneficiaries by decree »(10), in favor of an accelerated distribution of the vaccine.
» The head of state once again got carried away about the vaccination campaign in France, during a crisis meeting at the Élysée Palace, as reported in Le Point. « What is this stuff? », Emmanuel Macron thus launched, pointing to the 45-page guide for directors of Ehpad and USLD (long-term care units) for vaccination. « Who wrote this? The French take us for fools! » »(11).
The bureaucracy that is the hallmark of the state, and particularly of France, is being called into question by the person who represents it (who is its leader and emblem), while at the same time denying any possibility of fostering patient-doctor interaction.
« I want us to really speed up on vaccines. I don’t understand why a medical consultation is required before, blow that up! » the president continued. The High Authority of Health actually recommends a pre-vaccination medical consultation in addition to consent for nursing home residents. »(12)
The summit of technocracy is reached here when the only determining judgement(13), no longer reduced to a science but to a technique (vaccines), is imposed, for the good of all. And this, regardless of the singular trajectories and particular contexts. Figures are needed: after those of the deaths, those of the vaccinated!
The King vaccinates. His henchmen apply.
« I’ll have to consult my board about that, » replied an official from the High Authority for Health, present at the meeting. « Very well. If it is not possible to remove it, the French will know that it is because of the HAS, » Emmanuel Macron then launched. »(14)
The King threatens(15). His people are afraid.
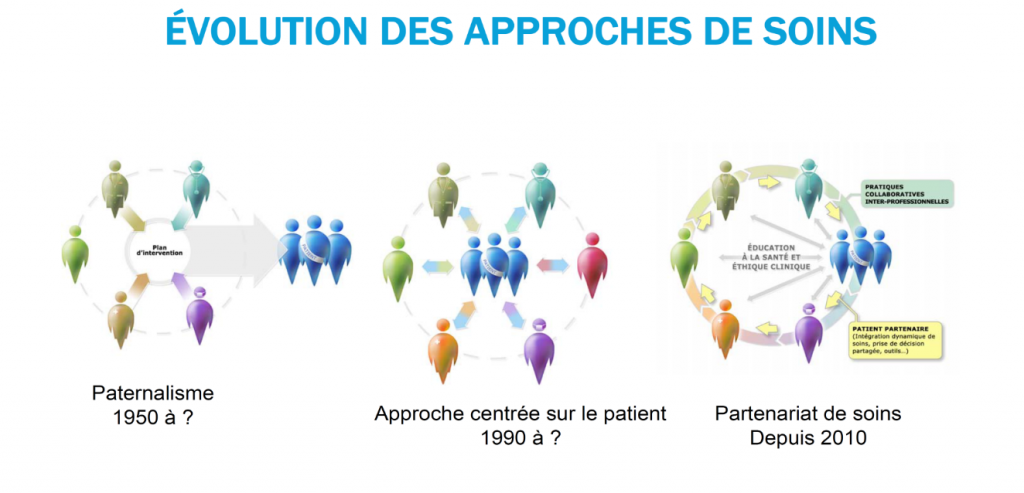
However, from an emancipatory point of view, what should deeply question the public health sector, and especially the health promotion sector and the whole population, is the issue shown in the figure below.
We find the different stages of a complex empowerment process that has been emerging very gradually over the last ten years in the health sector, that of the « patient-partner », which is described in the afterword to the book « Penser la formation des professionnels de la santé. Une perspective intégrative » testifies. The introductory paragraph is reproduced here(16):
» Isn’t it time to realize that people’s relationship with their health is changing rapidly, that patients and their families are no longer the same as they were ten, twenty or fifty years ago? The traditional image of the patient submitted to a benevolent and omniscient system, which assumes a total, unilateral and too often autocratic care, is slowly giving way to a more dynamic vision of a patient in search of information, who claims his singularity and his ontological need to move again despite the constraints of his condition « .
Some will argue the health emergency in order to allow a backtracking to the paternalistic model.
This health emergency is also pleaded to justify laws that are liberticidal with respect to constitutions and whose internal logic is criticized by the lawyers most committed to a systemic reflection about our democracies. Indeed, it is precisely at the time of crises that a real competence-in-situation (on the part of those in charge of all decisions) should make it possible to avoid losing resources (those of people’s capacities to act) in order to favor a partnership response, global, to the problem. However, this requires probity(17)That is to say, a coherence between what we say in a democracy and what we do.
Thus, complex, interprofessional and open thinking is a priority, leading to « problematizing » and understanding all the elements at stake, in order to preserve what is.
Starting with this model of care partnership, promoted and carried by those who have integrated into their care practices this capacity for partnership, including that of not restricting the power of the Other, that is to say, of preserving his autonomy.(18)
It is precisely such a paradigm that should be protected in order to serve as a beacon to avoid the authoritarian drift of which every emergency situation is the breeding ground…
However, the ever-present hegemony of a hospitalocentric, emergency, curative model (centered on healing and not on « care »), not integrated (because fragmented in its epistemological foundations (cf. Carte blanche(19)) is obviously in great collusion with such « top-down » discourses(20).
Thus, along with many other sectors of care (for example, mental health or facilities for people with disabilities, nursing homes), the palliative care community, which is struggling to gain recognition in the classic health care habitus(21)At the beginning of the health crisis, the Covid 19 literally disappeared, vanishing like a ship in the Bermuda triangle, with the appearance of the Loch Ness monster.(22)
This is all the more sad, in the sense of a very great sadness that overwhelms us as soon as we evoke this reality, this Living, that of the end of life…, that our elders needed it so much!
But, and we cannot forget this(23), « we are at war »!
This infantilization of medical interventions concerned both professional (prescribing, vaccinating, etc.) and non-professional target audiences. It was dramatically worsened by decisions about non-therapeutic interventions, such as containment.
We have seen a health system that, rather than « coming together » in the face of the threat, has appeared totally dislocated between two entities. On the one hand, a hospital medicine, presenting via the media a sophisticated technical platform. On the other hand, a general medicine, of proximity, reduced to a subaltern role, thus showing, in an extremely acute way, a recurrent symptom of our health system: that of the displayed contempt or, at least, of the non-recognition, within the medical world, of the general medicine but also, of what is called: the « paramedical »(24) (nurses, physiotherapists, osteopaths, logopedists, …). A logic well described in social psychology, that of the theories of intergroup conflict(25), has certainly taken root there(26). The technical issue (respirators in particular) was exacerbated by the media , reinforcing the stereotype of a necessarily technical, sophisticated and urgent medicine. As for the politicians, concerned exclusively with the tip of the iceberg, they have essentially used the submerged part of the health system for technical execution (PCR test, vaccination). All discriminatory phenomena begin with the development of stereotypes that are conducive to prejudice, and these stereotypes guide our behavior(27). Man is definitely not the master of his own house!
Thus, in addition to a medical logic that favours belief in the certainty of technoscience to the detriment of practice (white cards(28)), there is also a logic that values the pyramidal, vertical and hierarchical structure of the organization of health care, to the detriment of an integrative — global — vision of the health system. This has led to a real dismemberment of the latter, facilitated by this form of « desertion by regulation » that we have highlighted.
The lack of a comprehensive approach has not only affected the macro systemic level (health system), it has also affected the micro systemic level.
Indeed, considering the person in his or her entirety implies starting from a postulate that is necessarily non-reductive of the latter. However, » in the field of medical practice, now separated from any serious anthropological reflection, this cultural narrowing is hard felt: [… ] »(29). The anthropological perspective allows us to consider illness in three ways: illness as a natural category, emerging from the objectivist approach and the nosographic approach (Disease); illness as a subjective experience of the patient (Ilness) accessible through language and interpretation; and finally illness as a process of integration and social construction of the health problem (Sickness), culturally and historically situated. The French language, which in the common vocabulary is reduced to the use of the term « maladie », deprives itself of this nuance that the English language brings and that is underlined by the three terms in brackets.
Such an assumption allows us to develop a non-reductive conception of health and to get closer to the just the WHO definition of health ». Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.
Similarly, at the foundation of any self-respecting health organization, the primary health care approach(30) postulating the integration of: community health promotion; disease prevention; integration of curative services and integration of rehabilitation services, provides the necessary operational openness to this WHO definition.
Thus, by sweeping away everything in its path, the Covid reveals to us, for those who know how to listen, the global necessity of everything. Recalling that it is « It is impossible to know the parts without knowing the whole, nor to know the whole without knowing the parts in particular. Still with Pascal (31) and in order to avoid that « The eternal silence of these infinite spaces frightens me », and that once again fear prevails, only the development of a capacity for complex thought(32) will allow us to get out of the impasse, the fragmentation and the reductionism, where everything, at this moment, as E. Piaf sings « drags us and drags us along… ».
Such a project is a long-term, historical and cultural project, and can only be carried out with the lever of education.
From our perspective, it should take root where the soil for such abuses is most fertile, notably in the medical and health world, and flourish through the leverage of medical and health training.
« After the muscular speeches announcing the eradication of terrorism, here are the learned speeches on the « zero Covid ». And always the same obsession with security, the same dream of a world without risk, without crime and without disease. We would be delighted, if we did not know how easily the dream of a perfect world can turn into the nightmare of the societies of fear »(33).
Still, emancipation must be the project of the « present man ».
It is on the condition of a transformational — educational — aim that bodies, people and systems, at the next pandemic, will no longer dislocate themselves, like puppets, and Pinocchio not to recognize it.