By Reinfocovid Belgium and the ASBL « Notre Bon Droit » — Analysis by Marc G. Wathelet, Ph. (Molecular Biology)

Dear Mr. Vandenbroucke, Deputy Prime Minister and Minister of Social Affairs and Public Health
Thank you for your response to our letter regarding mandatory vaccination of caregivers*, which you justify on the basis of a number of assertions that are not supported by documentation of scientifically proven facts.
On the contrary, the scientific data available to date contradicts your entire argument and, as detailed below, we can only conclude that mandatory vaccination of caregivers is not only unnecessary, but also counterproductive from a public health point of view, beyond the fact that it violates the principles of bioethics and medical ethics, as well as human rights.
Mandatory vaccination of caregivers is unnecessary because studies show beyond a reasonable doubt that it neither prevents the contamination of an individual, nor reduces the viral load of infected persons, and thus their ability to transmit the virus to others.
In Appendix A you will find a long list of facts, scientific publications and official statements from qualified agencies and individuals, such as Dr. J. M. M. M., who has been involved in the study of the effects of climate change. Fauci, which confirms our assertion that vaccination does not prevent an individual from becoming infected and being able to transmit the delta variant circulating today to others.
We will only mention here the latest example: on September 23, the Irish Examiner announced that in the city of Waterford, 99.7% of people over 18 were fully vaccinated, the highest total in the European Union(1). On October 11, the Waterford News & Star reported that the city had the highest incidence rate in Ireland(2).
There is only one conclusion, which cannot be disputed in good faith: beyond the studies, in the real world, in practice, Vaccination does not prevent transmission of SARS-CoV‑2 within a community.
The message that COVID vaccines would be « safe and effective », a claim unsupported only by the absence of the necessary hindsight, has been hammered constantly for many months in all media. One of the negative effects of this campaign is the acceptance of this statement as an established fact, not only by the population but also by its leaders.
As a result, vaccinated people are less likely to follow barrier measures such as distancing themselves or wearing masks, and because they are more likely to be asymptomatic when infected, making them less aware of the risk they pose to others, they are actually more likely to spread the virus than unvaccinated people.
In practice, this means that the COVID Safe Ticket is not only useless but counterproductive: a license for vaccinated people to infect others, whether they are vaccinated or not.
The same reasoning applies to caregivers, even if they were more scrupulous in observing the barrier measures, because the effectiveness of these measures is only partial: vaccinating all caregivers will not prevent the contamination of « people who are sick or vulnerable because of their old age », which you are rightly concerned about.
We agree with you that « people in care are entitled to maximum security ». We propose two non-exclusive alternatives to mandatory vaccination of caregivers that will be much more effective in preventing nosocomial infections:
1. Have all health care personnel, vaccinated or not, tested at a high frequency. In this regard, it should be noted that nasopharyngeal testing is not without risk, as reported by the Academy of Medicine in France(3). Two other safer methods can be considered: an oro-pharyngeal antigen test or an oral PCR test.
2. Implement a voluntary ivermectin prophylaxis program: there are 14 studies that support the effectiveness of this approach(4).
Finally, mandatory vaccination of caregivers is counterproductive from a public health perspective because those who still refuse to be vaccinated will no longer be able to work, and therefore the number of caregivers, already limited, will be even more reduced, with a negative impact on public health. In France, there are ~300,000 unvaccinated caregivers (~10%)(5), and 15,000 of them are already suspended(6). In Belgian hospitals, 9.4% of caregivers are not vaccinated and in MR/MRS, 13.1% are not(7).
You state, « Scientists say that 70% of the total population (including children) would need to be fully vaccinated for everyone to be protected. With the Delta variant, which is more contagious than the earlier variants, we are still aiming for that 70%, but we are striving for the highest percentage possible. »
This opinion seems to be shared mainly by experts mandated by the government. On the contrary, many scientists had anticipated that vaccination during a pandemic would not be a sufficient approach to control the virus, and events have proven them right (see Appendix A for a list of citations).
You say that « Vaccination reduces the circulation of the virus ». This is contradicted by the articles cited above about the delta variant (Appendix A), the example of the city of Waterford, and now a large study shows that increases in COVID-19 are indeed not related to vaccination levels worldwide (a study of 68 countries, as well as 2947 counties in the United States)(8).
You say « If we are afraid of variants, we certainly need to vaccinate more today. » Since the objective data indicate that vaccination does not work in practice, even when everyone is vaccinated, the solution cannot be to vaccinate more!
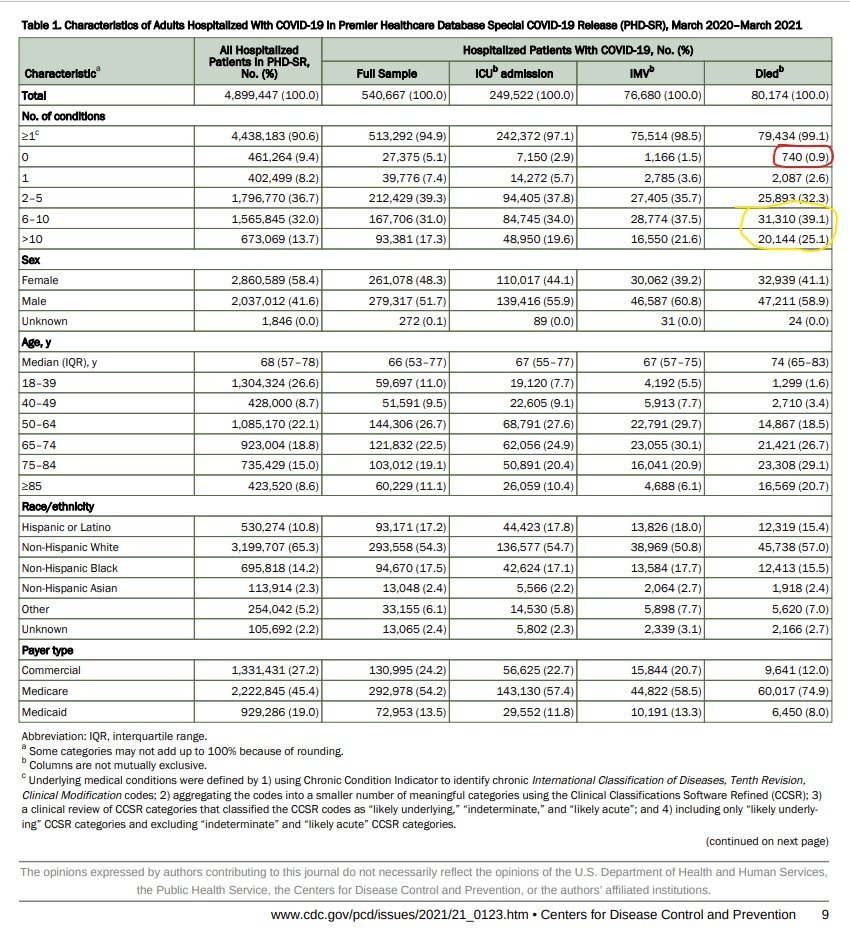
There is no reason to be afraid of the variants: on the one hand, the lethality of the delta variant is one-tenth of alpha according to Public Health England, and on the other hand, the lethality of COVID is inherently low. It is mostly related to the presence of comorbidities (99% of deaths occur in people with one comorbidity, 96% in people with multiple comorbidities, Appendix B).
Most importantly, this lethality is comparable to that caused by other respiratory infections. Therefore, neither the COVID Safe Ticket nor compulsory vaccination are justifiable from a public health point of view !
Those at risk have had the option of being vaccinated or can take prophylactic treatment if they choose not to be vaccinated. The situation of these individuals cannot therefore justify putting other healthy individuals at unnecessary risk.
The inherent risk of COVID vaccination in the medium and long term is simply unknown, due to lack of hindsight (although the prolonged post-vaccination syndrome, similar to long COVID, is noted). The short-term risk is clear despite the intense efforts of health authorities, mainstream media and GAFAM to suppress all information on this subject.
For example, the Israeli Ministry of Health posted an article on its Facebook page about severe adverse reactions that it described as very rare only to find itself inundated with a deluge of opposing opinions from its citizens (14,000 in a few hours), opinions that were simply deleted. Simply denying this reality is not a solution to the problem it poses.
Facebook routinely deletes any group that reports on vaccine adverse events, groups with tens of thousands of users in the United States and elsewhere. By what right? In the French-speaking world alone, the (non-exhaustive) collection of screenshots of these individual reports testifies to the catastrophic scale of the phenomenon(9).
All pharmacovigilance databases worldwide report an increase in severe adverse events and deaths for COVID vaccines ((10)(11)(12)[Royaume-Uni] (13) .
Analysis of VAERS data, for example, shows a much higher incidence for COVID than influenza vaccines of severe adverse events (28X more) and deaths (57X more, see Appendix B). What is the point of these pharmacovigilance sites if such figures are brushed aside as inconsequential, when on the contrary they call for the suspension of the vaccination campaign until their significance is established?
Fact-checking sites, funded by the pharmaceutical industry, come to the rescue of the doxa by claiming that there is no evidence that these deaths are attributable to vaccines. This is reversing the burden of proof!
According to a report from the ANSM in France (28.01.2021), the official rule in pharmacovigilance is that: « The analysis of reported cases takes into account clinical, chronological, semiological and pharmacological data. It can lead to the exclusion of the responsibility of the vaccine in the occurrence of an adverse event observed when another cause, certain, is highlighted.
In fact, an audit of VAERS data shows that only 14% of deaths following vaccination can be attributed to another cause; and not just anyone is making these reports, with 67% of the reports being made by a physician. Similarly, in Eudravigilance, 79% of reports of death were made by a health professional.
All Bradford Hill criteria are observed, implicating these vaccines as the cause of most reported adverse events. When autopsies, which are all too rarely done, are performed, between 30% and 100% of deaths are attributable to vaccination (see Appendix B).
These databases are poorly designed, leading to erroneous reports on both sides of the debate. For example, a figure of more than 25,000 deaths following vaccination against COVID is being circulated for Eudravigilance. A more rigorous analysis indicates 7,174 deaths as of October 9, 2021. VAERS analysis yields a number of deaths of the same order of magnitude (7,680, as of October 8, 2021).
These pharmacovigilance systems are passive, leading to a very significant under-reporting of the actual number of cases. A factor of 5 seems conservative, but regardless of the exact number, what is indisputable is that healthy, young people with no co-morbidities die as a result of vaccination or are severely injured.
The rotavirus vaccine was withdrawn from the market in 1999 because of only 15 cases of intussusception. The swine flu vaccination campaign in 1976 was stopped after 25 deaths. We are at least 3,000 times that (Appendix B). How many more deaths will it take before we face the facts?
The data show that those who are cautious about vaccines are more educated on average than those who favor vaccination, contrary to how they are portrayed in the media.
And the reality of serious adverse events due to vaccination is confirmed by the fact that it is precisely caregivers who do not want to be vaccinated, despite their education and the fact that they are generally in favor of vaccination (they are not antivaxers!), because they are on the front line and can see the damage that these vaccines cause.
It is therefore deeply immoral to make vaccination compulsory It is therefore immoral to make vaccination compulsory, whether it is for health care providers or for any other category of citizens. Similarly, it is contrary to bioethics to encourage vaccination of classes of individuals who were excluded from Phase 3 clinical trials, including pregnant women and those under 18 years of age.
Childhood deaths due to COVID are extremely rare and observed exclusively in individuals with severe co-morbidities, and therefore the deaths of healthy children already recorded following vaccination should lead to an immediate moratorium on the vaccination of children and pregnant women, in addition to the lack of hindsight on the long-term effects of this procedure on these populations.
Compulsory vaccination violates not only ethics, but also fundamental concepts of rights as demonstrated by Alessandro Negroni, professor of philosophy of law at the University of Genoa: » In the eyes of European and international law, genetic vaccines against cancer constitute medical experimentation on human beings. From both an ethical and legal point of view, no one can be forced to undergo a form of medical experimentation without free and informed consent.(14)
We hope you will consider this sourced analysis, and realize that the idea of mandatory vaccination with experimental products for anyone, and the implementation of a COVID Safe Ticket based on anything other than a recent test, should be abandoned.
Let us also abandon therapeutic nihilism, and treat infected individuals early, as medicine had always done before the beginning of this crisis.
With our deepest respect,
By Reinfocovid Belgium and the ASBL « Notre Bon Droit
Analysis by Marc G. Wathelet, Ph. (Molecular Biology)
The effect of vaccination on the risk of SARS-CoV‑2 infection and transmission to others was modest in the initial studies, but the rapid decline in immunity in the vaccinated individual and the emergence of more contagious variants makes this effect negligible today, as discussed in detail in this paper https://www.linkedin.com/pulse/questions-sur-limmunisation-et-la-transmission-de-marc-wathelet/?published=t, written in the context of a legal action by the ASBL « Notre Bon Droit » in opposition to the « COVID Safe Ticket » proposed by the Belgian Government.
This document is dated July 28, 2021, contains 50 references and the studies that have appeared since then only confirm this analysis:
https://www.medrxiv.org/content/10.1101/2021.07.28.21261295v1
https://onlinelibrary.wiley.com/doi/10.1111/joim.13372
https://www.medrxiv.org/content/10.1101/2021.08.19.21262139v1
https://www.medrxiv.org/content/10.1101/2021.08.12.21261951v2
https://www.cdc.gov/mmwr/volumes/70/wr/mm7031e2.htm?s_cid=mm7031e2_w
https://www.medrxiv.org/content/10.1101/2021.09.28.21264262v1.full.pdf
https://www.medrxiv.org/content/10.1101/2021.09.02.21262979v1
https://www.medrxiv.org/content/10.1101/2021.09.28.21264260v1.full.pdfhttps://link.springer.com/article/10.1007/s10654-021–00808‑7
https://www.nejm.org/doi/pdf/10.1056/NEJMoa2114583?articleTools=true https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(21)02183–8/fulltext
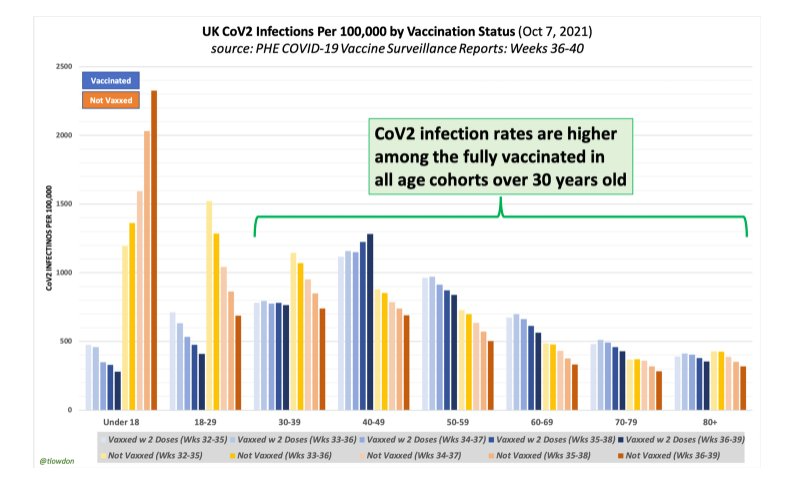
The most recent data from Public Health England indicate that in all cohorts the rate of infection is higher in the vaccinated than in the unvaccinated from age 30 onwards. Under these circumstances, mandatory vaccination is simply absurd.
The CDC and Dr. Fauci recognizes the impact of the higher contagiousness of the delta variant and reinstates masking for the vaccinated https://www.cnbc.com/2021/07/28/dr-fauci-on-why-cdc-changed-guidelines-delta-is-a-different-virus.html.
In addition, the document cited above https://www.linkedin.com/pulse/questions-sur-limmunisation-et-la-transmission-de-marc-wathelet/?published=t also compares immunity to SARS-CoV‑2 acquired following vaccination with that following natural infection and shows that the latter is more robust, broader, more balanced between antibody and T‑cell production, and lasts longer than vaccine immunity, resulting in better and longer-lasting protection against infection for convalescent individuals compared to vaccinated individuals.
Caregivers are among those who have been most exposed to the virus so far, so it would make no sense to force vaccination on them when their natural immunity is more effective. Here again, the studies that have appeared since then only confirm this analysis:
https://www.medrxiv.org/content/10.1101/2021.08.12.21261951v2
https://www.bmj.com/content/bmj/374/bmj.n2101.full.pdf
The #Covidrationnel collective in Belgium, which includes some thirty university professors, researchers and doctors, has conducted a similar analysis and reached the same conclusions: https: //covidrationnel.be/2021/10/06/de-source-sure/
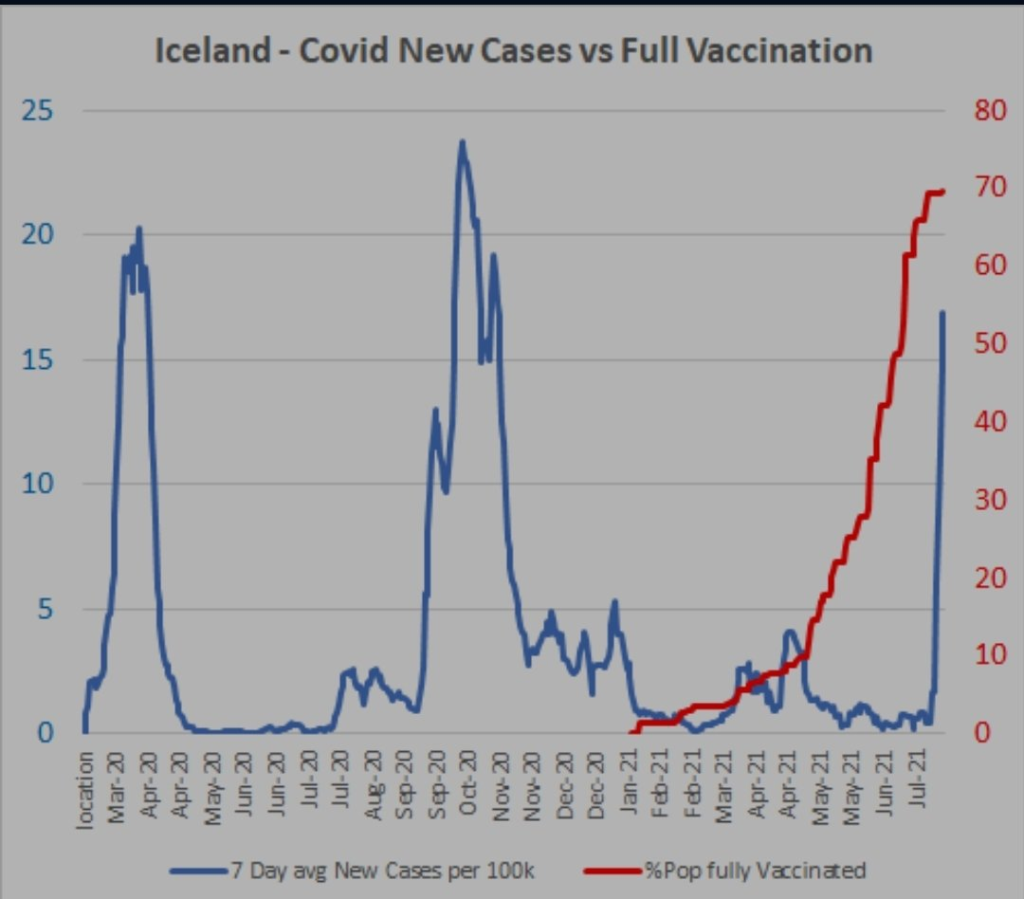
These studies are confirmed by observations in the real world, in the territories with the highest vaccination rate such as Seychelles, Gibraltar, Iceland, this high rate does not prevent important waves of contamination that follow closely the vaccination campaign.
More recently, in the city of Waterford in Ireland, where 99.7% of the population over 18 years of age is fully vaccinated, https://www.irishexaminer.com/news/arid-40704104.html, this city still has the highest incidence rate in Ireland (618.9 per 100,000 over the last 2 weeks) https://waterford-news.ie/2021/10/11/waterford-now-has-highest-incidence-of-covid-in-ireland/
A recent global study shows that increases in COVID-19 are indeed not related to vaccination levels worldwide (68 countries and 2947 counties in the United States) https://link.springer.com/article/10.1007/s10654-021–00808‑7.
COVID
It is not useful from a public health point of view to consider the general lethality rate, it is a question of identifying the populations at risk.
The dangers of COVID
The dangers of COVID are related to age and the presence of comorbidities, 99% of deaths occur in people with one comorbidity, 96% in people with multiple comorbidities according to the US CDC :
Survival rates at COVID by age group according to the team of Drs. Ioannidis:
Age Survival rate
0–19 99.9973%
20–29 99.986%
30–39 99.969%
40–49 99.918%
50–59 99.73%
60–69 99.41%
70+ 94.5%
These numbers do not distinguish COVID from other respiratory infections in terms of case fatality, and therefore do not warrant a different approach to managing this disease from a public health perspective. Therefore neither the COVID Safe Ticket nor the mandatory vaccination are justified from a public health point of view!
The dangers of vaccination against COVID
There are excellent vaccines, with a very favorable risk-benefit ratio, against severe diseases, such as tetanus or yellow fever. However, the benefit-risk ratio is sometimes unfavorable, and the vaccine in question is then withdrawn from the market.
For example, a rotavirus vaccine was withdrawn from the market in 1999 because of only 15 cases of intussusception https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC2094741/.
The swine flu vaccination campaign in 1976 was stopped after 25 deaths https://www.lemonde.fr/planete/article/2009/09/15/le-precedent-vaccinal-de-1976_1240713_3244.html. It also caused 532 cases of Guillain-Barré syndrome.
A simple correlation does not mean causation. The Bradford Hill criteria are used, which have been found to be largely verified for these vaccines as shown below, the list is :
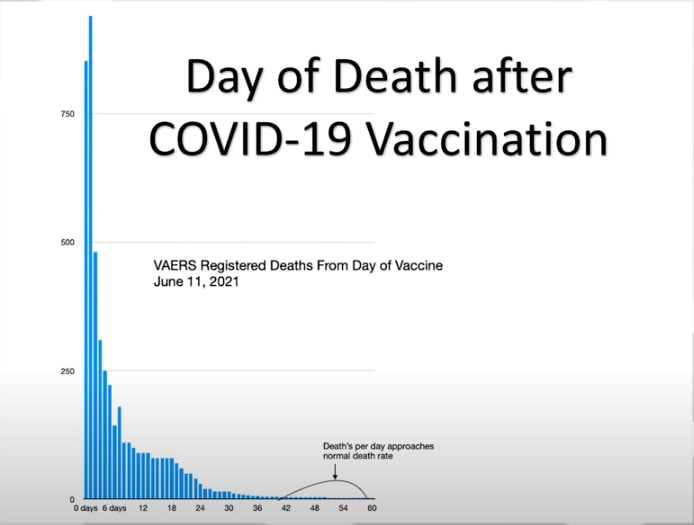
For example, temporality(#5) shows a very high incidence of death in the days following vaccination, before dropping back to normal levels.
The same pattern of adverse events is observed in Europe and the United States(#3), which are listed below in descending order of frequency from their respective standards:
pulmonary embolism, stroke, deep vein thrombosis, thrombosis, increased fibrin D dimers, appendicitis, tinnitus, cardiac arrest, death, Parkinson’s disease, slow speech, aphasia (inability to speak), fatigue, pericardial effusion, headache, chills, pericarditis, deafness, myocarditis, intracranial hemorrhage spontaneous abortion, cough, Bell’s palsy, paresthesia, blindness, dyspnea (difficulty breathing), myalgia, dysstasia (difficulty standing), convulsions, anaphylactic reaction, suicide, speech impediment, thrombotic thrombocytopenic purpura (TTP), paralysis, swelling, diarrhea, neuropathy, multivisceral dysfunction syndrome (MDS), depression.
Their number increases with the level of vaccination, and there is specificity (#4), the adverse event profile listed above is different from that observed for influenza vaccines but is similar to the effects of COVID; also, certain populations are affected differently, e.g., myocarditis and pericarditis affect young men more.
Biological plausibility (#7): COVID vaccines produce the SARS-CoV‑2 Spike protein in our cells as infection with the virus does, and the adverse effects resemble those seen in the disease; the Spike protein demonstrates intrinsic toxicity to cardiac endothelial cells and pericytes invitro: https://www.nature.com/articles/s41593-020–00771‑8
https://www.sciencedirect.com/science/article/pii/S096999612030406X?via%3Dihub
https://www.biorxiv.org/content/10.1101/2021.04.30.442194v1
https://www.biorxiv.org/content/10.1101/2020.12.21.423721v2
https://www.ahajournals.org/doi/10.1161/CIRCRESAHA.121.318902.
Experimental evidence (in animals or in humans, #8), experiments on mice reproduce myopericarditis https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciab707/6353927.
Strength of association(#1) and stability(#2):
Report of serious adverse events and deaths for all COVID vaccines per million doses compared with annual influenza vaccines from 2016 to 2021, the H1N1 influenza strain vaccine in 2009–2010, and all vaccines except COVID from 2006 to 2021 in the US VAERS system.

Analysis of VAERS data shows a much higher incidence for COVID than influenza vaccines of severe adverse events (28X more) and deaths (57X more).
Absolute numbers of serious adverse events and deaths in VAERS for the 3 vaccines in the United States against COVID, and their ratio per number of injections.
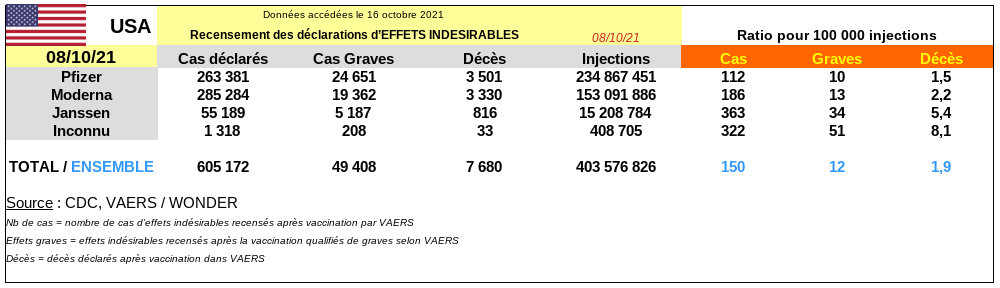
An audit of VAERS data shows that only 14% of deaths following vaccination can be attributed to another cause; at least 67% of reports were initiated by a physician.
Because the VAERS system is passive, only a small proportion of actual cases are recorded in it. This proportion can be estimated on the basis of a study of 64,900 employees of a Massachusetts hospital measuring severe reactions consistent with anaphylaxis that may occur immediately after vaccination: they occurred at a rate of 2.47 per 10,000 vaccinations. The incidence rate of confirmed anaphylaxis in this study is higher than that reported by CDC based on passive (VAERS) methods of spontaneous reporting (0.025–0.11 per 10,000 vaccinations). https://jamanetwork.com/journals/jama/fullarticle/2777417
These data suggest that underreporting in VAERS is by a factor of between 22.5 and 98.8!
This indicates that the number of deaths exceeds 150,000 and the number of severe adverse events exceeds one million in the United States.
Absolute numbers of serious adverse events and deaths in the European Economic Area for the 4 COVID vaccines, and their ratio per number of injections.
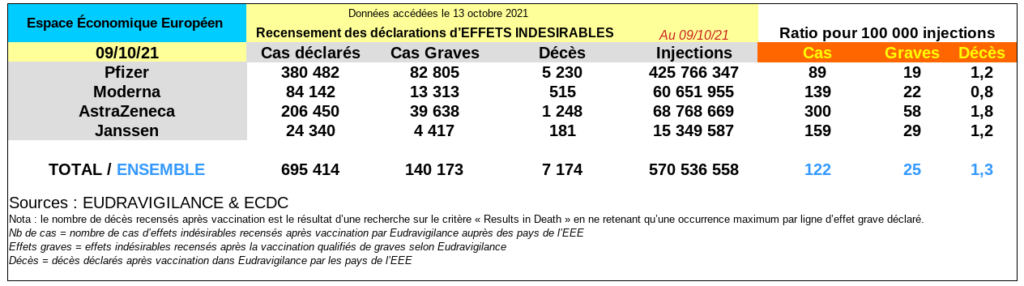
79% of the death reports were entered by a health care provider.
The official rule in pharmacovigilance: « The analysis of reported cases takes into account clinical, chronological, semiological, and pharmacological data. It can lead to the exclusion of the responsibility of the vaccine in the occurrence of an adverse event observed when another cause, certain, is highlighted.
When autopsies are performed, which are all too rarely done, between 30 and 100% of deaths are attributable to vaccination. Peter Schirmacher, chief pathologist at the University of Heidelberg, determined that autopsy reports indicate that at least 30 to 40 percent of a sample of 40 people who died within two weeks of vaccination actually died from the vaccine, being conservative https://www.aerzteblatt.de/nachrichten/126061/Heidelberger-Pathologe-pocht-auf-mehr-Obduktionen-von-Geimpften.
Forensic scientists Prof. Arne Burkhardt and Prof. Walter Lang presented the results of ten autopsies in Reutlingen on Monday, September 20. Of the ten deaths, seven are « probably » related to the injections, five of which are « very probably » related. For the last three cases, one remains to be evaluated, another appears to be « coincidental, » and for the last, the link « is possible but not certain. » https://tinyurl.com/3b779fer.
In Norway, when 23 vaccine-related deaths occurred in a nursing home, authorities performed 13 autopsies and all 13 deaths were found to be related to vaccination https://norwaytoday.info/news/norwegian-medicines-agency-links-13-deaths-to-vaccine-side-effects-those-who-died-were-frail-and-old/.
A French drug evaluation center concluded that vaccination against COVID should be discontinued https://tinyurl.com/2s64aenn, for all 4 products. And the Moderna vaccine has been abandoned by some countries for younger children (Norway, Sweden, Denmark; France for the second dose).
Finally, in an article entitled « Why do we vaccinate children against COVID? », the authors conclude that not only is their vaccination contraindicated, but that even for the most vulnerable subjects over 65 years of age, the risk-benefit analysis shows that there are 5 times more deaths attributable to vaccination than to the disease https://www.sciencedirect.com/science/article/pii/S221475002100161X.
It is contrary to bioethics and the law to vaccinate classes of individuals who were excluded from Phase 3 clinical trials, in particular those under 18 years of age. https://medcritic.fr/la-vaccination-des-enfants-contre-le-covid19‑1/: society, by vaccinating children, puts them at risk in order to protect adults without considering their well-being, whereas it is the responsibility of adults to protect themselves.
It is not only inaccurate that the delta variant would be more dangerous for children https://www.medrxiv.org/content/10.1101/2021.10.06.21264467v1, but data from the UK Office for National Statistics (ONS) shows a 46% increase in deaths in the 15–19 age group since vaccination was allowed (+63% in young men, +16% in young women #4 ), compared to the same period in 2020. https://theexpose.uk/2021/09/30/deaths-among-teenagers-have-increased-by-47-percent-since-covid-vaccination-began/.
The indigent response of Minister Vandenbroucke’s office: