What is the outcome of this epidemic episode? How effective are health measures?
This analysis is based on the Sciensano epidemiological report dated 30/11/2020(1)
Below we will analyze the epidemiological graphs of covid published by Sciensano, in order: 1 the number of cases, 2 and 3 hospitalizations, 4 intensive care patients, 5 mortality.
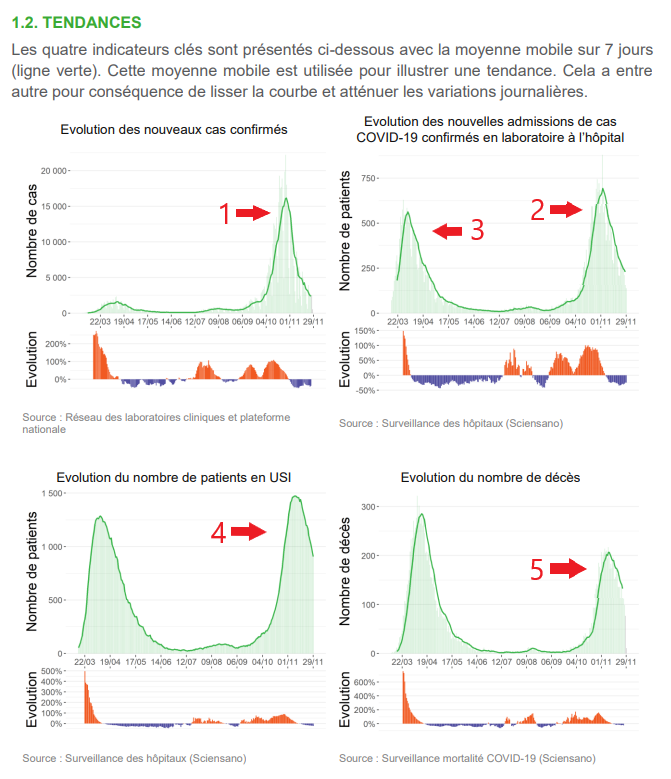
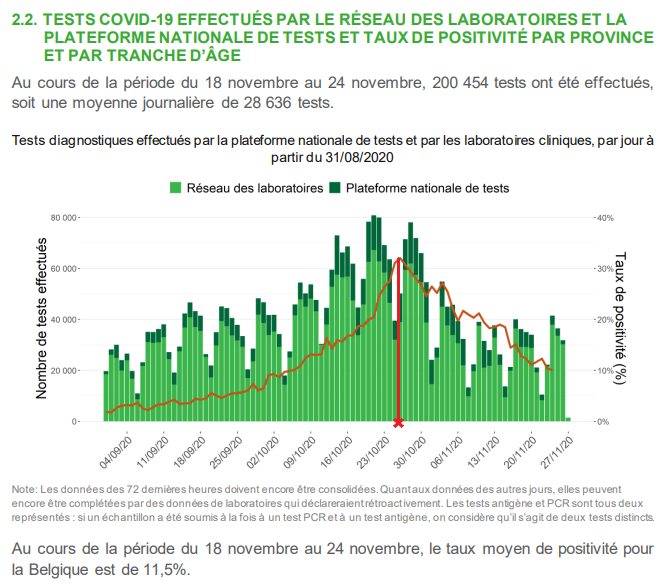
The decrease in the number of positive tests continues and falls below the 2,400 per day weekly average. They are not always « cases » in the clinical sense of the term and the majority have mild forms of the disease (95%). This peak of positives is in no way comparable to the one in March-April when only patients who arrived at the hospital in very advanced stages were tested. The number of tests performed is stabilizing at around 200,000 per week.
As the epidemic peak is coming to an end, we will be able to evaluate, later in this analysis, the different indicators since the beginning of this autumn episode.
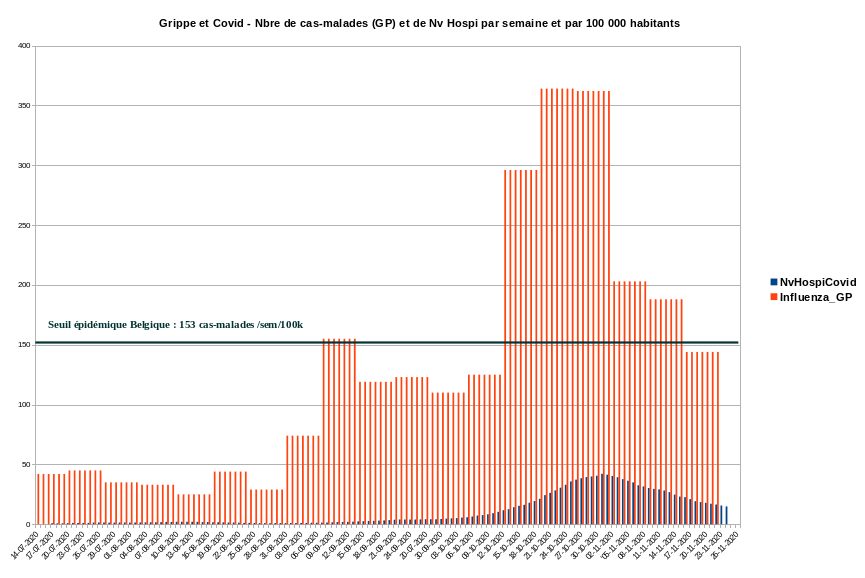
However, we can already put the importance of this epidemic into perspective by comparing the new hospitalizations attributed to covid with the number of « new influenza » declared by the sentinel system, based on general practitioners. Both are expressed per week and per 100,000 inhabitants in the graph below published by Christophe de Brouwer, professor at the School of Public Health of the ULB. The visualization immediately gives orders of magnitude of the problem related to acute respiratory infections, which includes sars-cov‑2. We use covid hospitalizations as a benchmark and not identified « cases » because of the questionable reliability of the PCR detection method, which we will discuss in Section 3.
The curve for hospitalizations classified as « covid » also continues to fall. What we can say in numbers about the peak of this epidemic:
The threat exposed by the experts that led the political authorities to tighten the health measures during the month of October is that of hospital saturation. Although the situation was indeed very tense in the covid units, it is clear that the hospitals were not saturated! Attributing this inflection to health measures taken by the authorities is completely misleading. Indeed, the epidemic peak of this autumnal episode seems to have been reached around October 23, as shown in the perspective of week 44(4).
This can be seen in the Sciensano graph below where a major parameter of the quantification of the epidemic episode, namely the covid test positivity rate, peaks around October 25.
While it is commonly accepted that there is usually a 10–15 day delay between sanitary measures taken to limit the spread of sars-cov2 and its expected effects(5), the impact of this new containment on the evolution of the epidemic is highly questionable, if not absolutely non-existent. At most, one could attribute a possible effect of the measures taken at the beginning of October, but this remains to be demonstrated. Nevertheless, the most coercive measures taken after the second half of October cannot be the cause of the inflection of the indicators observed in November. Most obviously, this autumn epidemic peak was expressed through the various indicators in the form of a banal bell curve on which the restrictions imposed on the population probably had little effect.
Is this fall epidemic of the same magnitude as the first one? A priori, the peak of hospitalizations exceeds that of March, but the mortality as well as the lethality of this episode are lower. In addition, the onset of seasonal respiratory illnesses (fall/winter) implies more suspected clinical cases of covid. PCR tests, with their very high sensitivity and non-absolute specificity, will not always distinguish covid from other seasonal respiratory infections.
It is important to note that depending on the sensitivity of PCR tests, positive tests for sars-cov2 may have no medical significance when systematized to this extent. Indeed, some studies show a very high proportion of clinically irrelevant positives when the number of PCR amplification cycles (CT) exceeds 30(6). And in Belgium, the number of PCR amplification cycles (CT) ranges from 30 to 35(7).
Recently, a study published in the journal Clinical Infectious Diseases(8) has shown, through experiments of sars-cov2 viral cultures from patients tested positive by PCR, that beyond 30 TC there are 70% of positive tests for which the virus cannot be cultured because the traces detected are non-viable, and therefore not contagious. From 35 CT onwards, 97% of the positive tests show that there is no live virus!
This raises huge questions about the reliability of RT-PCR tests to determine whether a person is sick or even contagious.
If the CT cycles of the PCRs performed are too high, the tests are hypersensitive and therefore cannot determine, even if positive, whether the patient is indeed sick with covid.
All these patients labelled « covid », whether they really have this disease or not, will in fact cause a rapid saturation of the hospital system because of the cumbersome protocol of their care.
Add to that the fact that some patients admitted for anything other than covid, undergo PCR tests, and if they are positive, they are listed as « covid hospital admission »!
Even more eloquent is this article from the Corman-Drosten Review Report(9) which points out 10 major scientific flaws at the molecular and methodological level of the RTPCR test to detect sars-cov2!
The conclusion of this article mentions, and I quote, the « enormous flaws and design errors of the PCR protocol… » Enough to seriously question this diagnostic tool!
What would be the origin of this covid outbreak?
The number of patients in intensive care units (ICUs) is also decreasing. The number of « covid » patients in the ICU reached a peak of 1,475 throughout the country. This is about 70% of the capacity of intensive care beds in Belgium (about 2,000).
As for the saturation of the intensive care units in Belgium, unfortunately this is not an exceptional situation either. According to Dr. Philippe Devos, intensivist at the CHC Liège, during the peak of the flu epidemic in January/February 2020, the ICU bed occupancy rate was over 90%! And this by patients who developed complications from severe influenza(14).
It is also imperative to highlight the fact that covid clinical pictures are significantly less bleak than in March/April. The proportion of ventilated patients has clearly decreased, intubations are only done as a last resort and now constitute only 60% of the management of patients in ICU compared to more than 80% in March/April. This improvement in terms of « severity » of cases is most certainly due to better management of patients upstream thanks to a more thorough knowledge of the disease as well as the introduction of treatments such as anti-coagulants, corticosteroids or oxygen therapy, which reduce ICU visits and their severity.(15)
And this is confirmed by a lower covid mortality at the present time.
The « covid » mortality is now also decreasing, the intensity of this peak is 34% less than the previous one.
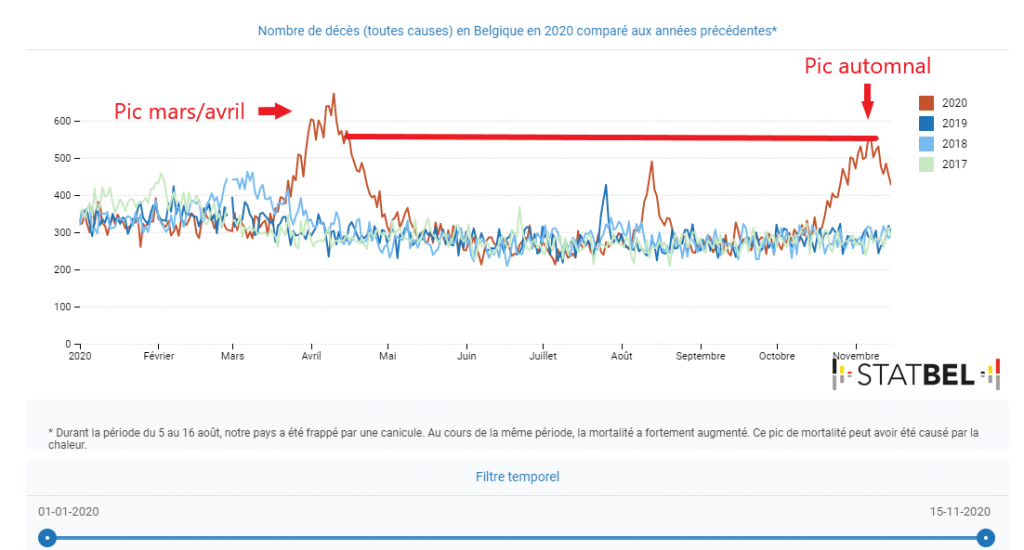
Fortunately, there was less covid mortality than during the previous episode, which is a major proof of a lesser severity of this episode. I therefore refer you to the graph below which concerns the general mortality data for Belgium: there is, until November 15, a notable excess of general mortality with regard to this autumn 2020 epidemic episode compared to previous years, but less important than in March/April.
There is no doubt that this episode has caused a significant excess of mortality in Belgium. But what about our neighbors where the same sars-cov2 was in circulation?
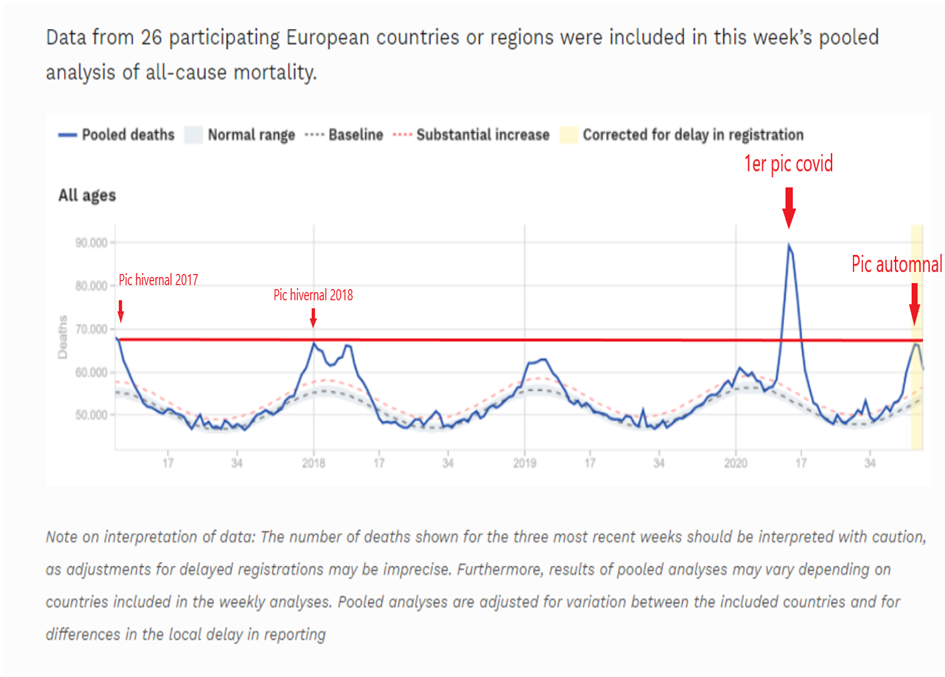
At the European level, globally, in terms of impact on overall mortality, this epidemic episode is much less important than the first one and is of the order of a winter flu episode as can be seen on this graph of mortality data collected among 26 European countries(17).
It is deplorable to note that among all our neighboring countries, Belgium has the highest lethality rate after France, on which, moreover, our leaders are often quick to copy decisions in the field of health policies.
The apparent case-fatality rate (deaths over cases) for covid in Belgium is 2.95%, compared with 1.59% for Germany, 1.72% for the Netherlands and 0.92% for Luxembourg. Only France has a rate close to Belgium with 2.38%.(18)
It should be remembered that the actual case fatality rate of the disease is estimated at between 0.3 and 0.65% by the WHO and the US CDC(19)(20).
In doing so, it would be a good time to question the strategies for managing this health crisis, given the dramatically disastrous results displayed by the Kingdom in comparison with its neighbors. The latter have a comparable sociology, standard of living and demography.
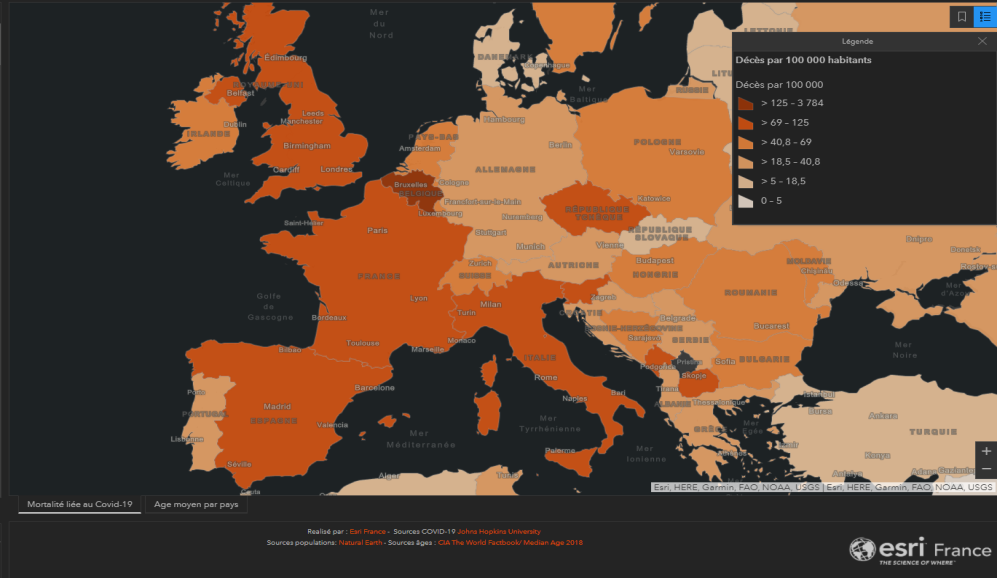
Here is a European map of covid mortality per 100.000 inhabitants.
And Belgium appears in dark orange with the sad world record of 144 covid deaths per 100 000 inhabitants!
The health management policy in Belgium must be questioned. First of all, are the drastic containment measures really effective?
Let’s compare the graphs of excess mortality (nbp17) of countries that have adopted the containment strategy versus others that are more flexible in this matter. The first are countries that have applied strict and generalized containment measures: France, Spain, Austria and Belgium. The second are neighboring and comparable countries that have not applied containment, or have applied it in a localized or even relaxed manner: Germany, Portugal, Hungary and the Netherlands.
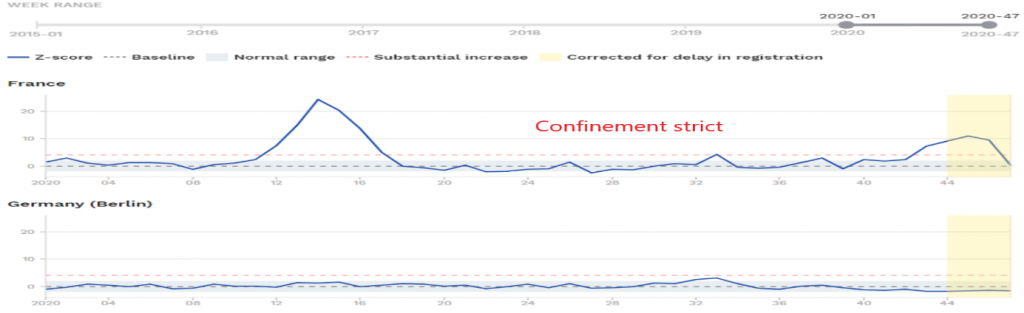
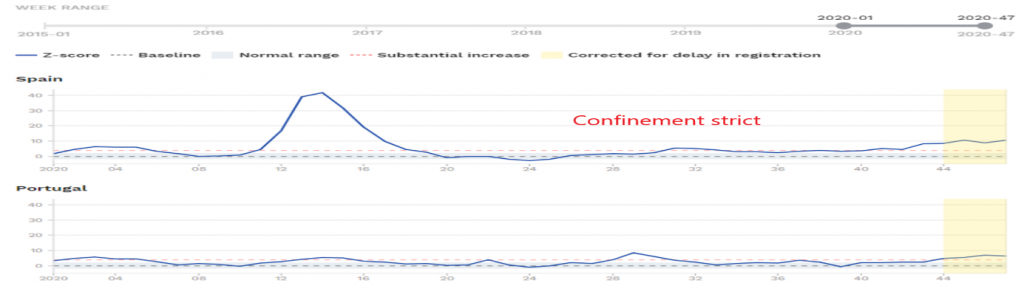
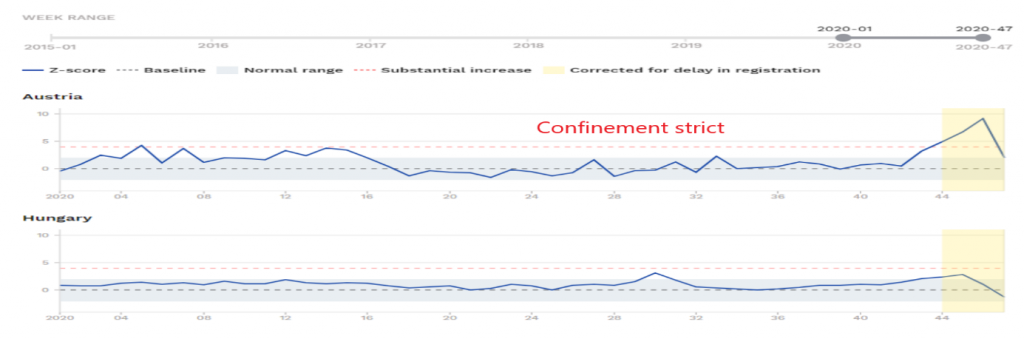

Without jumping to conclusions, it cannot be said from this brief comparison that the containment policy has a clear impact on overall mortality.
In fact, the effectiveness of containment has not been demonstrated: the countries that have drastically applied this measure are among those with the most catastrophic per capita mortality rates in Europe: Belgium, Spain, Italy, United Kingdom and France. Add to this that a seroprevalence study conducted by the Spanish authorities on more than 60,000 subjects showed that confined people were more contaminated than people who continued their professional activities in the essential sectors. Data, confirmed by another Italian study, which may legitimately cast doubt on the containment strategy as a solution to the epidemic(22)(23).
Furthermore, the evidence for the ineffectiveness of confinement on overall mortality seems to be confirmed by the French study of IRMES in collaboration with the University of Toulouse. Researchers analyzing data from 188 countries around the world over 9 months found no correlation between harsh health measures and reduced mortality, with some evidence pointing in the opposite direction (nbp13). The collateral damage of the most restrictive health strategies, such as containment, seems to tip the balance in favor of risks rather than benefits. As shown by several British studies which highlight an unprecedented increase in late diagnosed cancers and heavy consequences on untreated pathologies such as cardiovascular accidents. Not to mention suicides, depression and the resurgence of domestic violence(24).
Hospitalization rate (number of hospitalizations per identified case): 4.81
Proportion of hospitalized patients admitted to intensive care: 20%(0.96% of cases)
Proportion of resuscitation patients on ventilators: 60%(0.58% of cases)
Apparent case fatality rate for the fall episode (since September 15): 1.4
Median age of death: 83 years
In conclusion, it seems very likely that sars-cov2 takes on a seasonal pattern and that a particular variant is responsible for this fall epidemic peak. Contrary to what the media-political doxa would like to distill, this upsurge in the epidemic is not due to a « new epidemic ».It is a classic, identifiable and quantifiable evolution of the dynamics oftheviral epidemic, which depends on a series of variables in which human behavior does not seem to be as decisive as the media-political expertocracy would have us believe.
If the peak of the sars-cov2 epidemic in Belgium took place during week 43 (around October 25), i.e. before the most coercive measures taken by the authorities at the end of October, this raises a huge doubt about the efficiency and legitimacy of the governmental sanitary measures. Not to mention the huge confession, collected by a VRT journalist, from the Minister of Health Franck Vandenbroucke, who mentions, and I quote: » a « psychological » measure » when referring to the decision to close non-essential businesses(25)! This is enough to make the many citizens who have suffered from this decision cringe.
In a reckless headlong rush, our government, supported by this unanimous and dogmatic expertocracy, will have, without really analyzing the situation, plunged the people into a new confinement that will most certainly have heavy consequences. Not to mention the fact that the restrictive measures taken in the past may even have contributed to the intensity of this epidemic episode!
One thing is certain: faced with the same virus, our Dutch, German and Luxembourg neighbors fared much better than we did, which undoubtedly reflects a problem of consistent management of the crisis. As Belgium is a very poor performer in terms of mortality and lethality at the European level, it seems legitimate to question the validity of sanitary measures that give little results. To support this criticism, a striking statement by Richard Horton, editor of the prestigious medical journal The Lancet, who said on Monday, November 16, » This typically Belgian system has not worked, it has failed. We could have avoided most of these 14,000 deaths. People have died because of the political organization » ! Absolutely eloquent, this release speaks for itself(26)!
Against all odds, the political and media apparatus, not content with not questioning these sanitary measures, shamelessly continues to pour into a dialectic that makes the citizen feel guilty, tacitly making the latter solely responsible for the evolution of the epidemic as well as for the tensions in the hospitals. The latter, which could, in the opinion of many practitioners, be avoided if early management and prophylaxis protocols were put in place on an outpatient basis(27)(28).
It seems mixed without being dramatic at the European level, but it is totally catastrophic for Belgium in comparison with its neighbors. This is probably due to a calamitous political management of the situation.
What can we conclude about the effectiveness of the health measures taken by our government?
In view of the evidence we have been able to follow, it is clear that there is at least a lack of evidence that restrictive measures such as curfews, business closures and general containment are effective. One could even see a risk-benefit bias without, moreover, having a significant impact on overall mortality.
This is a serious reason to hold our political leaders accountable!
Thank you for reading.
Annes Bouria, pharmacist, member of the Transparency-Coronavirus collective
https://www.transparence-coronavirus.be